![]()
Medical Terminology Daily (MTD) is a blog sponsored by Clinical Anatomy Associates, Inc. as a service to the medical community. We post anatomical, medical or surgical terms, their meaning and usage, as well as biographical notes on anatomists, surgeons, and researchers through the ages. Be warned that some of the images used depict human anatomical specimens.
You are welcome to submit questions and suggestions using our "Contact Us" form. The information on this blog follows the terms on our "Privacy and Security Statement" and cannot be construed as medical guidance or instructions for treatment.
We have 354 guests and no members online
")
Marcia Crocker Noyes
(1869 – 1946)
Further to my comment on old books and research that started with an interesting bookplate (Ex-Libris). I continued my research and found that the person in charge of the Osler library bookplate was a fascinating individual that today maybe a ghost in the MedChi library and building in Baltimore... This is certainly an article that can be called "A Moment in History"
Marcia Crocker Noyes was the librarian at The Maryland State Medical Society from 1896 to 1946 and was a founding member of the Medical Library Association.[1][2][3]
Sir William Osler, MD. a famous Johns Hopkins surgeon was a noted bibliophile and had a large personal collection of books on various topics. When he became the President of MedChi in 1896, he was dismayed at the condition of the library and knew that with the right person and some stewardship, it could become a significant collection. Sir William asked his friend, Dr. Bernard Steiner, a physician and President of the Enoch Pratt Free Library in Baltimore for suggestions of a librarian, and Dr. Steiner recommended Marcia Crocker Noyes. A native of New York, and a graduate of Hunter College, Marcia had moved to Baltimore for a lengthy visit with her sister, and took a “temporary” position at the Pratt Library, which turned into three years. Although she had no medical experience or background, she was enthusiastic, and most importantly, she was willing to move into the apartment provided for the librarian, who needed to be available 24 hours a day.
The image in this article is Ms. Noyes on her first year on the job. Marcia developed a book classification system for medical books, based on the Index Medicus, and called it the Classification for Medical Literature. The system uses the alphabet with capital letters for the major divisions of medicine and lower-case ones for the sub-sections. The system was used for many years, but it's now dated and the Faculty's original shelving scheme was never changed. The card catalogs still reflect her classification and many of the cards are written in Marcia's back-slanting handwriting.
Marcia knew enough to ask the Faculty's members about medical questions, terminology and literature. She gradually won over the predominantly male membership and they became her greatest allies; Sir William at the start, and then for nearly 40 years, Dr. John Ruhräh, a wealthy pediatrician with no immediate family of his own. She made a point of attending almost every Faculty function, and in 1904, under guidelines from the American Medical Association, Marcia was made the Faculty Secretary. For much of her first 10 years, she was the Faculty's only full-time employee, only being assisted by Mr. Caution, the Faculty's janitor. Later in life Marcia would say that she hired him because of his name!
Within ten years, the library had outgrown its space, and plans, spearheaded by Marcia and Sir William before his move to Oxford, were made to build a headquarters building, mainly to house the library's growing collection of medical books and journals.
Marcia was instrumental in the design and building of the new headquarters. She travelled to Philadelphia, New York and Boston to look at their medical society buildings, and eventually, the Philadelphia architectural firm, Ellicott & Emmart was selected to design and build the new Faculty building. Every detail of the building held her imprimatur, from the graceful staircase, to the light-filled reading room, and all of the myriad details of the millwork, marble tesserae, and most of all, the four-story cast iron stacks. She was on-site, climbing up unfinished staircases, checking out the progress of the building, which was built in less than one year at a cost of $90,000.
Among the features of the new building was a fourth-floor apartment for her. She referred to it as the "first penthouse in Baltimore" and it had a garden and rooftop terrace. The library collection eventually grew to more than 65,000 volumes from medical and specialty societies around the world. Journals were traded back and forth, and physicians eagerly anticipated the arrival of each new issue. At the same time, Marcia was involved in the Medical Library Association as one of eight founding members. The MLA promotes medical libraries and the exchange of information. One of the earliest mandates of the MLA was the Exchange, a distribution and trade service for those who had duplicates or little-used books in their collections. Initially, the Exchange was run out of the Philadelphia medical society, but in 1900 it was moved to Baltimore and Marcia oversaw it. Several hundred periodicals and journals were received and sent each month, a huge amount of work for a tiny staff. In 1904, the Faculty had run out of room to manage the Exchange, so it was moved to the Medical Society of the Kings County (Brooklyn). But without Marcia's excellent administrative skills, it floundered and in 1908, the MLA asked Marcia to take charge once again.
In 1909, when the new Faculty building opened, there was enough room to run the Exchange and with the help of MLA Treasurer, noted bibliophile and close friend, Dr. John Ruhräh, it once again became successful. Additionally, Marcia and Dr. Ruhräh combined forces to revive the MLA's bulletin, which had all but ceased publication in 1908, taking the Exchange with it. This duo maintained editorial control from 1911 until 1926. In 1934, around the time of Dr. Ruhräh's death, Marcia became the first “unmedicated” professional to head the MLA. During her tenure, the MLA incorporated, the first seal was adopted, and the annual meeting was held in Baltimore. Marcia wanted to write the history of the MLA once she retired from full-time work at the Faculty, but her health was beginning to fail. She had back problems and had suffered a serious burn on her shoulder as a young woman, possibly from her time running a summer camp, Camp Seyon, for young ladies in the Adirondack Mountains. In 1946, a celebration was planned to honor Marcia's 50 years at the Faculty. But she was adamant that the physicians wait until November, the actual date of her 50 years. However, they knew she was gravely ill, and might not make it until then, so a huge party was held in April. More than 250 physicians attended the celebration, but the ones she was closest to in the early years, were long gone. She was presented with a suitcase, a sum of money to use for travelling, and her favorite painting of Dr. John Philip Smith, a founder of the Medical College in Winchester, Virginia. It was painted by Edward Caledon Smith, a Virginia painter who had been a student of the painter Thomas Sully.[4] She adored this painting and vowed, jokingly, to take it with her wherever she went.
The painting was not to stay with her for very long, for she died in November 1946, and left it to the Faculty in her will. Her funeral was held in the Faculty's Osler Hall, named for her dear friend. More than 60 physicians served as her pallbearers, and she was buried at Baltimore's Green Mount Cemetery. In 1948, the MLA decided to establish an award in the name of Marcia Crocker Noyes. It was for outstanding achievement in medical library field and was to be awarded every two years, or when a truly worthy candidate was submitted. In 2014, the Faculty began giving a bouquet of flowers to the winner of the award in Marcia's name, and in honor of her work. Much evidence exists for this tradition, as we know that the physicians, especially Drs. Osler and Ruhräh, frequently gave her bouquets of flowers. Marcia also cultivated flower gardens at the Faculty and decorated the rooms with her work.
Today, the MedChi building is open for tours and if the rumors are to be believed Ms. Marcia Crocker Noyes is still at work in her beloved library as the "resident ghost" [1][5]

NOTE: This article has been modified from the original Wikipedia article on Marcia Crocker Noyes. The article itself is well-written with interesting images of the subject. I would encourage you to visit it. The second insert is from book 00736 in my personal library and shows in pencil, the incredibly small handwriting of Marsha C. Noyes.
Sources:
1. "Marcia, Marcia, Marcia" MedChi Archives blog.
2. "Marcia C. Noyes, Medical Librarian" (PDF). Bulletin of the Medical Library Association. 35 (1): 108–109. 1947. PMC 194645
3. Smith, Bernie Todd (1974). "Marcia Crocker Noyes, Medical Librarian: The Shaping of a Career" (PDF). Bulletin of the Medical Library Association. 62 (3): 314–324. PMC 198800Freely accessible. PMID 4619344.
4. Edward Caledon BRUCE (1825-1901)"
5. Behind the scenes tour MedChiBuilding
"Clinical Anatomy Associates, Inc., and the contributors of "Medical Terminology Daily" wish to thank all individuals who donate their bodies and tissues for the advancement of education and research”.
Click here for more information
- Details
This is a series of articles on depression and published as a community service. The information in these articles follow our Privacy and Security Guidelines and cannot be construed as medical guidance. For additional information and counseling, consult with your physician or the appropriate health care professional of your choice. You can also find information on Transcranial Magnetic Stimulation (TMS) here. For the initial article on this series click here.
There are several forms of depressive disorders.
• Major depression: Characterized by the presence of severe symptoms that interfere with the individual's ability to work, sleep, study, eat, and enjoy life. An episode can occur only once in a lifetime, but more often, a person has several episodes separated by varying lengths of time.

Click for a larger image
• Persistent depressive disorder: Also known as Major Depressive Disorder (MDD) it is a depressed mood that lasts for at least 2 years. A person diagnosed with persistent depressive disorder may have episodes of major depression along with periods of less severe symptoms, but in general the depressive mood lasts for a minimum of 2 years. In both cases, patients present with depressed mood, loss of interest or pleasure, decreased energy, feelings of guilt or low self-worth, abnormal patterns of sleep or appetite, gruesome nightmares, and poor concentration.
Some forms of depression are slightly different, or they may develop under unique circumstances. They include:
• Psychotic depression: Psychotic depression occurs when a person has severe depression plus some form of psychosis, such as having disturbing false beliefs or a break with reality (delusions), or hearing or seeing upsetting things that others cannot hear or see (hallucinations).
• Postpartum depression: This is much more serious than the "baby blues" that many women experience after giving birth, when hormonal and physical changes and the new responsibility of caring for a newborn can be overwhelming. It is estimated that 10 to 15 percent of women experience postpartum depression after giving birth. There is a rare variant of this disorder, the prepartum depression, which as the name implies happens in the final stages of pregnancy. In both these cases the problem is that the patient cannot be treated with drugs as they may affect the fetus, or the patient cannot breast-feed the newborn eliminating an important stage in the mother-child bonding process. A depressed mother with drug therapy and concurrent side-effects may not able to care for her baby. Thia patient is a good candidate for TMS.
• Seasonal affective disorder (SAD): Is characterized by the onset of depression during the winter months, when there is less natural sunlight. The depression generally lifts during spring and summer. SAD may be effectively treated with light therapy, but nearly half of those with SAD do not get better with light therapy alone. Antidepressant medication and psychotherapy can reduce SAD symptoms, either alone or in combination with light therapy. In some patients the onset of SAD can be the trigger for MDD.
• Bipolar disorder: Also called manic-depressive illness, is not as common as major depression or persistent depressive disorder. Bipolar disorder is characterized by cycling mood changes that range from extreme highs (e.g., mania) to extreme lows (e.g., depression).
References:
1. Altshuler LL, Hendrich V, Cohen LS. Course of mood and anxiety disorders during pregnancy and the postpartum period. Journal of Clinical Psychiatry, 1998; 59:29.
2. Rohan KJ, Lindsey KT, Roecklein KA, Lacy TJ. Cognitive-behavioral therapy, light therapy and their combination in treating seasonal affective disorder. Journal of Affective Disorders, 2004; 80:273–283.XX
Next: Treatment options
- Details
The medical term [ictal] arises from the Latin word [ictus] meaning a "a blow, strike, stroke, or thrust," and [icere] meaning "to strike, to hit," also related to [iæcere], meaning "to throw". The root term is [ict-] and with the adjectival suffix [-al] means “pertaining to a blow or stroke”.
The use of the term [ictus] today refer to a sudden onset of medical or physiological event such as a seizure, stroke, headache, or migraine.
Associated terms are:
[Preictal] (sometimes written pre-ictal) meaning “before the blow or stroke” and usually refers to symptoms or signs that precede or are at the beginning of the ictus. These symptoms are also called a [prodrome].
[Postictal] (sometimes written post-ictal) meaning “after the blow or stroke” and refers to the period immediately after the ictus where the symptoms and signs are receding.
In the case of an epileptic seizure the [postictal state] is the altered state of consciousness after the seizure, and is characterized by drowsiness, confusion, nausea, hypertension, headache or migraine, and can be followed by amnesia.
- Details
The following article was published by Theo Dirix in his blog. He is one of the Vesalius Continuum project members and a contributor to this website. Theo Dirixis an author and a taphophile. He has successively held the office of Consul in Embassies of Belgium in Tanzania, Saudi Arabia, Jordan, Canada, the United Arab Emirates and, since 2011, Greece. His current posting is in Kopenhagen, Denmark Before 1989, he worked for the Flemish Radio 3 and commented on (mainly Moroccan) literature. He is constantly writing travel stories of his visits to cemeteries and graves. He is also the author of the book "In Search of Andreas Vesalius: The Quest for the Lost Grave".

Theo Dirix
“Andreas Vesalius is a rock star in well defined circles”, a friend wrote to me in an e-mail and: ”I hate disappointing people". That is to say with the results of the upcoming crucial phase in the search for his lost grave in Zakynthos, Greece. I guess she considers all 800 friends of my Vesalius Continuum Page as members of those "well defined circles". Let me assure her, and all of you, Vesalius groupies, that nobody will be disappointed.
Potential sponsors definitely won’t. They just have to ask Agfa HealthCare Greece, that has financed the Geographical Information System of the first phase. With the amount paid, a company cannot even buy a single add in a newspaper; Agfa got dozens of adds instead, during our talks, in publications and in this paragraph.
Neither will Vesalius groupies, even after a generous contribution to the crowd funding campaign. Beyond the pleasure of discovering a geophysical prospection, they can bid on the miniature facial reconstruction we will present here soon. Or on paintings of skulls, cells and blood; one of my mentors is already labeling his acrylic studies we will auction soon.
And finally, no scientist will. Of course, there are some who will grin if we find ... nothing, but they seem to forget that a non-discovery can be as important as a find. Many more, however, continue to encourage us. They know funerary slabs have already been found under the corner house of Kolyva/Kolokotroni in the city center, where we concentrate our search. I’ll never forget the reaction of an archaeologist when I showed her the pictures of those artefacts in Pavlos Plessas’s blog.
From pampalaia.blogspot.dk/2012/08/blog-post.html I quote:
"How many excavations would you say have taken place at this site, which could, and should, have been the focus of a universal cultural pilgrimage? As far as I know none! Unless of course the dynamites and the bulldozers that after the catastrophic earth-quakes of 1953 demolished any wall left standing and pushed it into the sea can be thought of as an archaeological dig."
Back to our plans: a team of four or five researchers will walk through that part of the town with a Ground Penetrating Radar device. They will drill small holes (of about one cm in diameter and twenty cm in depth) in the asphalt roads, pavements and surroundings to enter electrodes and carry out the Electrical Resistivity Tomography. To get permits for making the holes, have plans of any utility networks and carry out the fieldwork, this geophysical prospection will take five days maximum. After processing the survey, the research center IMS/FORTH, Rethymnon, will come up with a map of underground architectural remains.
How exiting is that? I'm looking forward to receiving your comments. Are you ready to register, to pledge your support ?
Personal note: Click on the following link to collaborate with this incredible quest. I already did. Dr. Miranda
GoFundMe Campaign for the next stage of the project
- Details
GoFundMe Campaign for the next stage of the project
A group of researchers and investigators are looking to the incredible possibility of finding the grave of Andreas Vesalius. Initially this led to the 2014 meeting "Vesalius Continuum" in the island of Zakynthos, Greece. At that time Dr. Sylviene Déderix, Pascale Pollier, and Theo Dirix presented the status of the research that led to identification of the location of the church where Vesalius was buried. This was the church of Santa Maria delle Grazie which would have been located in the northern sector of the modern town, around the current junction of Kolokotroni and Kolyva streets.
More on this original stage on the project was published on the following article: In Search of Andreas Vesalius, The Quest for the Lost Grave - The Sequel. Supporters for this research include world-renown scholars such as Prof. Omer Steeno and Dr. Maurits Biersbrouck, which appear in the video
The next stage in this quest is to perform a detailed analysis of the grounds around the church using Electrical Resistive Tomography (ERT) and Ground Penetrating Radar (GPR) as well as other non-invasive ground-sensing modalities. This kind of research is not cheap and requires funding.
Pascale and the research team have set a GoFundMe campaign to raise €9,900, roughly US$10,800, and I am asking all of the Vesalius followers and anatomy enthusiasts to contribute as little or as much as you can to make this next stage of the project a reality. You can reach the GoFundMe page here.
The video in this article is by courtesy of Vimeo.com
- Details
This is a series of articles on depression and published as a community service. The information in these articles follow our Privacy and Security Guidelines and cannot be construed as medical guidance. For additional information and counseling, consult with your physician or the appropriate health care professional of your choice. You can also find information on Transcranial Magnetic Stimulation (TMS) here. For the initial article on this series click here.
The medical term meaning "cause" is [etiology]. As you talk to a physician or research on the causes of depression knowing this term will come in handy. Most likely, the etiology of depression is a combination of genetic, biological, environmental, and psychological factors.
Depressive pathologies are disorders of the brain. Brain-imaging technologies, such as Magnetic Resonance Imaging (MRI), have shown that the brains of patients who have depression are physically different than those of non-depressed individuals. This is important to understand. A depression patient is not a "mental" or "crazy" person in the fact that there is an underlying physical brain disorder causing the depression. They are not "faking it" and the treatment must look into getting the brain back into a normal physical pattern.
The following images show a Positron Emission Tomography (PET) scan of both a non-depressed and a depressed individuals. In these images the areas of the brain involved in mood, thinking, sleep, appetite, and behavior appear different. These images do not reveal why the depression has occurred, only that a depressed brain is physically different from a non-depressed brain.
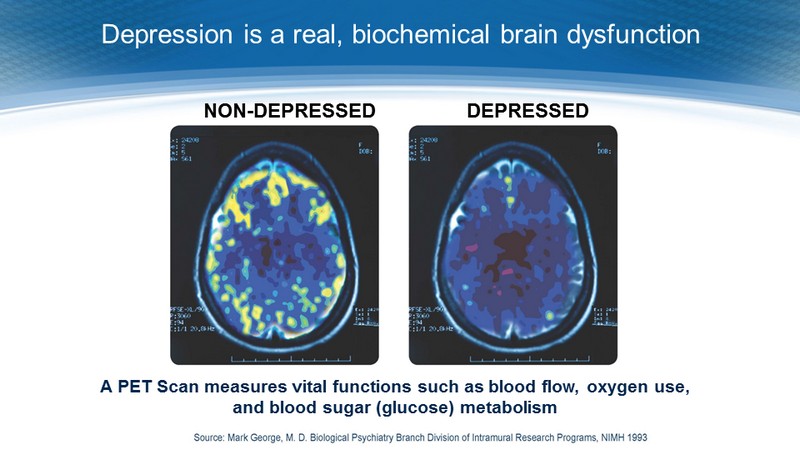
Click on the image for a larger view
Some types of depression tend to run in families, indicating a genetic base for the pathology. However, depression can occur in people without family history of depression. Scientists are studying certain genes that may make some people more prone to depression. Some genetics research indicates that risk for depression results from the influence of several genes acting together with environmental or other factors. In addition, trauma, the loss of a loved one, a difficult relationship, long winter seasons, or any stressful situation may trigger a depressive episode. Other depressive episodes may occur with or without an obvious trigger.
Who is at risk?
Major depressive disorder is one of the most common mental disorders in the United States. Each year about 6.7% of U.S adults experience major depressive disorder. Women are 70 % more likely than men to experience depression during their lifetime. Non-Hispanic blacks are 40% less likely than non-Hispanic whites to experience depression during their lifetime. The average age of onset is 32 years old. Additionally, 3.3% of 13 to 18 year olds have experienced a seriously debilitating depressive disorder.
Depression also may occur with other serious medical illnesses such as heart disease, stroke, cancer, HIV/AIDS, diabetes, and Parkinson's disease. People who have depression along with another medical illness tend to have more severe symptoms of both depression and the medical illness, more difficulty adapting to their medical condition, and more medical costs than those who do not have co-existing depression. Treating the depression can also help improve the outcome of treating the co-occurring illness
Source: National Institute of Mental Health
Next article: Types of Depression
- Details
BRRRRRRRR!!
A reminder of one of the joys of summer! The term [sphenopalatine ganglioneuralgia] is a fancy medical term for "brain freeze". which happens when we eat or drink very cold food.
The etymology of the term is complex. [Sphen-] is a term meaning "wedge" and refers to the sphenoid bone. [-palatine-] means "pertaining to the palate" (and to the bones related to the hard palate].
The root term [-gangli-] refer to a ganglion, which is a concentration of neuronal bodies, neurons being the main cells of the nervous system. [-neur-] means "nerve", and the suffix [-algia] means "pain". Simply said, the term [sphenopalatine ganglioneuralgia] means "nerve pain of the sphenopalatine ganglion".
The sphenopalatine ganglion (Meckel's ganglion, nasal ganglion or pterygopalatine ganglion) is a parasympathetic ganglion found in the pterygopalatine fossa. It is largely innervated by the greater petrosal nerve (a branch of the facial nerve); and its neuronal axons innervate the lacrimal glands and nasal mucosa.
Not everybody accepts this theory. Some state that "brain freeze" occurs because of rapid cooling of the blood in the pharynx, causing a drop of temperature of the internal carotid artery, which in turn causes cooling and pain in the meninges related to the base of the cranium.
My thanks to Gina Burg, for bringing this term to my attention. Dr. Miranda
Thanks to Forrest J. Bonjo for the image and additional information. The article was originally stored at pdu.edu, but the server was closed. If you click on the image, this will take you to the article stored at web.archive.org.