![]()
Medical Terminology Daily (MTD) is a blog sponsored by Clinical Anatomy Associates, Inc. as a service to the medical community. We post anatomical, medical or surgical terms, their meaning and usage, as well as biographical notes on anatomists, surgeons, and researchers through the ages. Be warned that some of the images used depict human anatomical specimens.
You are welcome to submit questions and suggestions using our "Contact Us" form. The information on this blog follows the terms on our "Privacy and Security Statement" and cannot be construed as medical guidance or instructions for treatment.
We have 118 guests and no members online
")
Marcia Crocker Noyes
(1869 – 1946)
Further to my comment on old books and research that started with an interesting bookplate (Ex-Libris). I continued my research and found that the person in charge of the Osler library bookplate was a fascinating individual that today maybe a ghost in the MedChi library and building in Baltimore... This is certainly an article that can be called "A Moment in History"
Marcia Crocker Noyes was the librarian at The Maryland State Medical Society from 1896 to 1946 and was a founding member of the Medical Library Association.[1][2][3]
Sir William Osler, MD. a famous Johns Hopkins surgeon was a noted bibliophile and had a large personal collection of books on various topics. When he became the President of MedChi in 1896, he was dismayed at the condition of the library and knew that with the right person and some stewardship, it could become a significant collection. Sir William asked his friend, Dr. Bernard Steiner, a physician and President of the Enoch Pratt Free Library in Baltimore for suggestions of a librarian, and Dr. Steiner recommended Marcia Crocker Noyes. A native of New York, and a graduate of Hunter College, Marcia had moved to Baltimore for a lengthy visit with her sister, and took a “temporary” position at the Pratt Library, which turned into three years. Although she had no medical experience or background, she was enthusiastic, and most importantly, she was willing to move into the apartment provided for the librarian, who needed to be available 24 hours a day.
The image in this article is Ms. Noyes on her first year on the job. Marcia developed a book classification system for medical books, based on the Index Medicus, and called it the Classification for Medical Literature. The system uses the alphabet with capital letters for the major divisions of medicine and lower-case ones for the sub-sections. The system was used for many years, but it's now dated and the Faculty's original shelving scheme was never changed. The card catalogs still reflect her classification and many of the cards are written in Marcia's back-slanting handwriting.
Marcia knew enough to ask the Faculty's members about medical questions, terminology and literature. She gradually won over the predominantly male membership and they became her greatest allies; Sir William at the start, and then for nearly 40 years, Dr. John Ruhräh, a wealthy pediatrician with no immediate family of his own. She made a point of attending almost every Faculty function, and in 1904, under guidelines from the American Medical Association, Marcia was made the Faculty Secretary. For much of her first 10 years, she was the Faculty's only full-time employee, only being assisted by Mr. Caution, the Faculty's janitor. Later in life Marcia would say that she hired him because of his name!
Within ten years, the library had outgrown its space, and plans, spearheaded by Marcia and Sir William before his move to Oxford, were made to build a headquarters building, mainly to house the library's growing collection of medical books and journals.
Marcia was instrumental in the design and building of the new headquarters. She travelled to Philadelphia, New York and Boston to look at their medical society buildings, and eventually, the Philadelphia architectural firm, Ellicott & Emmart was selected to design and build the new Faculty building. Every detail of the building held her imprimatur, from the graceful staircase, to the light-filled reading room, and all of the myriad details of the millwork, marble tesserae, and most of all, the four-story cast iron stacks. She was on-site, climbing up unfinished staircases, checking out the progress of the building, which was built in less than one year at a cost of $90,000.
Among the features of the new building was a fourth-floor apartment for her. She referred to it as the "first penthouse in Baltimore" and it had a garden and rooftop terrace. The library collection eventually grew to more than 65,000 volumes from medical and specialty societies around the world. Journals were traded back and forth, and physicians eagerly anticipated the arrival of each new issue. At the same time, Marcia was involved in the Medical Library Association as one of eight founding members. The MLA promotes medical libraries and the exchange of information. One of the earliest mandates of the MLA was the Exchange, a distribution and trade service for those who had duplicates or little-used books in their collections. Initially, the Exchange was run out of the Philadelphia medical society, but in 1900 it was moved to Baltimore and Marcia oversaw it. Several hundred periodicals and journals were received and sent each month, a huge amount of work for a tiny staff. In 1904, the Faculty had run out of room to manage the Exchange, so it was moved to the Medical Society of the Kings County (Brooklyn). But without Marcia's excellent administrative skills, it floundered and in 1908, the MLA asked Marcia to take charge once again.
In 1909, when the new Faculty building opened, there was enough room to run the Exchange and with the help of MLA Treasurer, noted bibliophile and close friend, Dr. John Ruhräh, it once again became successful. Additionally, Marcia and Dr. Ruhräh combined forces to revive the MLA's bulletin, which had all but ceased publication in 1908, taking the Exchange with it. This duo maintained editorial control from 1911 until 1926. In 1934, around the time of Dr. Ruhräh's death, Marcia became the first “unmedicated” professional to head the MLA. During her tenure, the MLA incorporated, the first seal was adopted, and the annual meeting was held in Baltimore. Marcia wanted to write the history of the MLA once she retired from full-time work at the Faculty, but her health was beginning to fail. She had back problems and had suffered a serious burn on her shoulder as a young woman, possibly from her time running a summer camp, Camp Seyon, for young ladies in the Adirondack Mountains. In 1946, a celebration was planned to honor Marcia's 50 years at the Faculty. But she was adamant that the physicians wait until November, the actual date of her 50 years. However, they knew she was gravely ill, and might not make it until then, so a huge party was held in April. More than 250 physicians attended the celebration, but the ones she was closest to in the early years, were long gone. She was presented with a suitcase, a sum of money to use for travelling, and her favorite painting of Dr. John Philip Smith, a founder of the Medical College in Winchester, Virginia. It was painted by Edward Caledon Smith, a Virginia painter who had been a student of the painter Thomas Sully.[4] She adored this painting and vowed, jokingly, to take it with her wherever she went.
The painting was not to stay with her for very long, for she died in November 1946, and left it to the Faculty in her will. Her funeral was held in the Faculty's Osler Hall, named for her dear friend. More than 60 physicians served as her pallbearers, and she was buried at Baltimore's Green Mount Cemetery. In 1948, the MLA decided to establish an award in the name of Marcia Crocker Noyes. It was for outstanding achievement in medical library field and was to be awarded every two years, or when a truly worthy candidate was submitted. In 2014, the Faculty began giving a bouquet of flowers to the winner of the award in Marcia's name, and in honor of her work. Much evidence exists for this tradition, as we know that the physicians, especially Drs. Osler and Ruhräh, frequently gave her bouquets of flowers. Marcia also cultivated flower gardens at the Faculty and decorated the rooms with her work.
Today, the MedChi building is open for tours and if the rumors are to be believed Ms. Marcia Crocker Noyes is still at work in her beloved library as the "resident ghost" [1][5]

NOTE: This article has been modified from the original Wikipedia article on Marcia Crocker Noyes. The article itself is well-written with interesting images of the subject. I would encourage you to visit it. The second insert is from book 00736 in my personal library and shows in pencil, the incredibly small handwriting of Marsha C. Noyes.
Sources:
1. "Marcia, Marcia, Marcia" MedChi Archives blog.
2. "Marcia C. Noyes, Medical Librarian" (PDF). Bulletin of the Medical Library Association. 35 (1): 108–109. 1947. PMC 194645
3. Smith, Bernie Todd (1974). "Marcia Crocker Noyes, Medical Librarian: The Shaping of a Career" (PDF). Bulletin of the Medical Library Association. 62 (3): 314–324. PMC 198800Freely accessible. PMID 4619344.
4. Edward Caledon BRUCE (1825-1901)"
5. Behind the scenes tour MedChiBuilding
"Clinical Anatomy Associates, Inc., and the contributors of "Medical Terminology Daily" wish to thank all individuals who donate their bodies and tissues for the advancement of education and research”.
Click here for more information
- Details
This article is part of the series "A Moment in History" where we honor those who have contributed to the growth of medical knowledge in the areas of anatomy, medicine, surgery, and medical research.
This is the continuation of the article “The Ephraim McDowell House and Museum (2)”. For the first article, click here.
The “Operating Room”
The so-called “operating room” is the place where everybody thinks a historical surgical event took place. The room is at a different level and communicates with the master bedroom. There is a plaque placed there byt Chapter XI of the Colonial Dames of America. In the room there is antique furniture and surgical instruments of the time.These are most probably not Dr. McDowell’s instruments, but I would like to believe so.
In the instrument kits you can clearly see different types of knives, lancets, needles, trephines, tourniquets, and amputation saws. What is interesting is that at the time (1809) there were no concepts of asepsia or anesthesia. So why did this historical operation did not get infected? Dr. McDowell’s habits and the location of the room may provide an answer. It is said that Dr. McDowell was very strict about bodily and environmental cleanliness (clothes and such). The location of the operating room is directly above the kitchen and has a separate set of stairs that leads directly to it. In the 1800's white linen was boiled.

The operating room
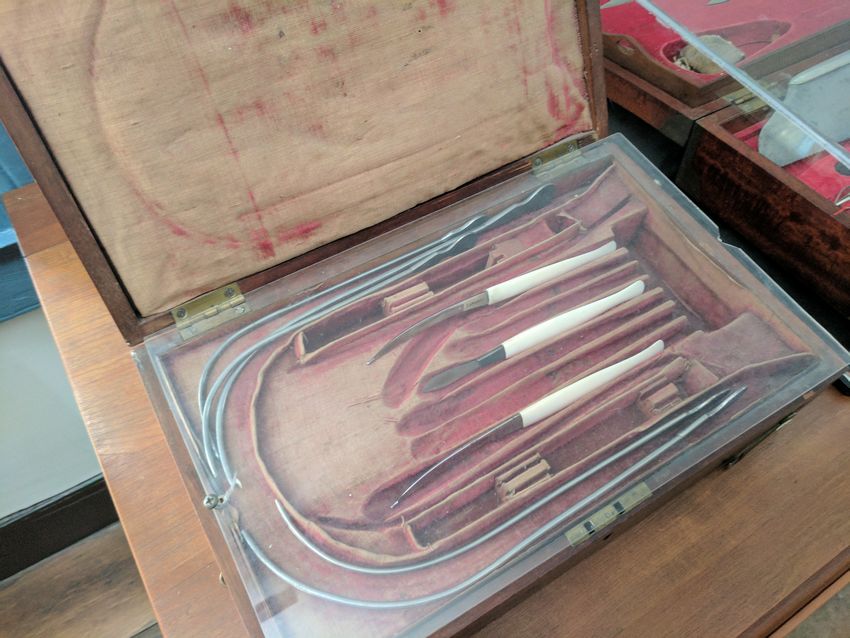
Surgical kit
In my opinion, this room was not only the “operating room” but also the “convalescent room” for people that were operated by Dr. McDowell. A room that served as pre and postoperatory, as well as an operating room.
In the room there are also additional artifacts, one of which definitely caught my attention: A doctor’s saddle bag. Since all transportation was by horse or buggy, a young doctor needed a special saddle bag that contained surgical instruments, medicine, and all that was needed for a home visit. This reminds me of a book I strongly recommend: “The horse and buggy doctor” by Arthur E. Hertzler, MD who was born almost 40 years after Dr. McDowell died.
The operation
Dr. McDowell visited Jane Todd Crawford in early December 1809 at her home 60 miles away. The reason was that two doctors wanted him to help in the birthing, as they thought the patient was pregnant and in pain. After examination Dr. McDowell explained to the patient that she had an (at the time) inoperable ovarian tumor and the she had a fatal prognosis. He also explained that he would be willing to try a risky and experimental surgery, but only at his home in Danville, KY. Mrs. Crawford agreed, as this was the only opportunity to save her life.
Mrs. Crawford, traveled very slowly for several days on horseback, crossing several rivers in the process. When she arrived she was tired and in a delicate condition, so she stayed several days before Dr. McDowell attempted the operation.
The operation itself has been described countless times. On Sunday December 25th, 1809 the patient was placed on a table in the “operating room”. Dr. James McDowell, a nephew assisted in the operation. He repeatedly asked his uncle to desist in the attempt that he was convinced was going to fail, the other physician attending was Dr. Alban Gilpin Goldsmith (1795 - 1876).
The patient was given some opioids (not anesthesia), her face was covered with a light piece of cloth and while she recited psalms and sang hymns Dr. Ephraim McDowell cut a 9-inch left paramedian incision opening her abdomen. The tumor was so big that it had to be cut open initially to partially drain a “dirty, mucous content”. After a single ligature through the broad ligament and infundibulopelvic ligament, the tumor was removed. It weighed 22 and a half pounds (10.2 kgs)! The incision was closed with an interrupted suture.

Surgical kit

Doctor's saddlebag
Five days after the operation, when Dr, McDowell came from the master bedroom to the now “postoperative” guest room he was surprised to see Mrs. Crawford on her feet making her bed! In Dr. McDowell’s own recounting of the procedure, the patient stayed with the McDowell family for 25 days after which she then again horseback rode 60 miles back to her home, in the middle of winter. Apparently these two protagonists never met again and Mrs. Crawford survived Dr. McDowell for at least 13 years. More information on the patient can be found in this article.
Dr. McDowell was a very religious man and the night before the operation he wrote a prayer that he kept in his pocket during the operation. Following is the text of the prayer. If you visit a store across the street from the McDowell House and Museum you can buy a facsimile of the prayer.
The Prayer
"Almighty God be with me I humbly beseech Thee, in this attendance in Thy holy hour; give me becoming awe of Thy presence, grant me Thy direction and aid, I beseech Thee, that in confessing I may be humble and truly penitent in prayer, serious and devout in praises, grateful and sincere, and in hearing Thy word attentive, and willing and desirous to be instructed. Direct me, oh! God, in performing this operation, for I am but an instrument in Thy hands, and am but Thy servant, and if it is Thy will, oh! spare this poor afflicted woman. Oh! give me true faith in the atonement of Thy Son, Jesus Christ, or a love sufficient to procure Thy favor and blessing; that worshipping Thee in spirit and in truth my services may be accepted through his all-sufficient merit. Amen."
Plaque on the operating room
Dr. McDowell only published the operation and its results in 1817. In several biographies that I have read it is stated that many were envious and jealous of his accomplishments to the point of creating tales that he “cut women open to murder them”. In her granddaughter’s biography or her illustrious grandfather she writes: “McDowell was conscious at the time he was doing the operation, that an angry and excited crowd of men were collected in the street awaiting the result of his experiment of "butchering a woman," as they expressed it. Had she died under the operation, there was no law in those primitive days sufficiently strong to have protected him from the people who were clamoring for his life—determined men who would have shown no mercy, for they regarded it a duty to avenge the wrong inflicted on Mrs. Crawford. Indeed his life hung on the recovery of the heroic woman.”
NOTE: Not long after I wrote this article, I came across a biography book of Dr. McDowell; inside it I found a copy of this prayer owned by Dr. Robert Thompson, along with a copy of a letter From Dr. McDowell addressed to Dr. Thompson with a description of the procedure.
Sources:
1. “Ephraim McDowell and Jane Todd Crawford, the Bicentennial of a Surgical Masterpiece” Benigno, BB Obst & Gynecol (2009) 113. 5:1141-1144
2. “The Biography of Ephraim McDowell, M.D.; The Father of Ovariotomy” Ridenbaugh, MY, 1890 CL Webster & Co.
3. “Ephraim McDowell: "Father of ovariotomy" and founder of abdominal surgery, with an appendix on Jane Todd Crawford” Schachner, A 1921, J.B. Lippincott Co.
- Details
The following is an article published by Theo Dirix in his blog. He is one of the Vesalius Continuum project members and a contributor to this website. Theo Dirixis an author and a taphophile. He has successively held the office of Consul in Embassies of Belgium in Tanzania, Saudi Arabia, Jordan, Canada, the United Arab Emirates and, since 2011, Greece. His current posting is in Kopenhagen, Denmark Before 1989, he worked for the Flemish Radio 3 and commented on (mainly Moroccan) literature. He is constantly writing travel stories of his visits to cemeteries and graves. He is also the author of the book "In Search of Andreas Vesalius: The Quest for the Lost Grave".

Theo Dirix
Isn’t it amazing how much we know about a scientist and physician who lived five hundred years ago, I am referring, of course, to the prominent figure of Andreas Vesalius (1514-1564)? (2)
After a jump start in academia in Italy, the Flemish anatomist made a sudden career move and became the family physician of Charles V, Emperor of the Holy Roman Empire, and to his successor Philip II and their powerful entourage in Spain. His brilliant early work, De Humani Corporis Fabrica Libri Septem, a milestone in the transition to empiric research, which has a revolutionary pedagogical and artistic approach, still inspires.
Isn’t it even more amazing that new discoveries about this giant and his achievements steadily continue to surface?(3) Most amazing, though, is that several hoaxes, mainly about his final months and days, doggedly survive.(4) Where is that undeniable proof that he ever ran into the otherwise so well documented inquisition?(5) Vesalius left Spain as a pious pilgrim. A laissez-passer [safe passage document] by Philip II and letters from the Spanish Embassy in Venice are conserved in archives in Spain. Even the thanking note by the Custodian of the Holy Places in Jerusalem, which Vesalius was to hand over to Philip II, reached its destination.(6) That unequivocally refutes the other obstinate prank that a shipwreck during his return was the cause of his death.

Santa Maria delle Grazie
Some now argue that scurvy may have been the cause; Omer Steeno, Maurits Biesbrouck and Theodoor Goddeeris point in the direction of general fatigue.(7) Obviously, only the discovery of his remains will help determine why he collapsed on the quay of Zakynthos (Greece), then a Venetian colony, as described in a recently rediscovered eyewitness report.(8) He was buried in the local catholic church of Santa Maria delle Grazie. Several Jerusalem pilgrims have indeed described his epitaph. Unfortunately, the church has disappeared. During its history, it was sacked, abandoned, damaged and finally, after major earthquake in 1953, bulldozed into the sea.
In view of the quincentenary of the anatomist, medical artist Pascale Pollier, hoping to reconstruct his face from his cranium, started a romantic quest for his remains. Under the impetus of the author and the Embassy of Belgium in Athens, archaeologists have been involved: Prof. Jan Driessen, Université Catholique de Louvain (UCL) and Director of the Belgian School in Athens, EBSA, and Apostolos Sarris, Deputy Director of the Institute for Mediterranean Studies - Foundation for Research and Technology, Hellas (IMS-FORTH).
In 2014, Dr. Sylviane Déderix (UCL/IMS-FORTH) checked the presumed location of the church through the spatial analysis of a Geographical Information System (GIS). With that digital tool, she displayed, corrected and analysed historical maps on modern cartographic data. The result confirms that the ruins of the Santa Maria delle Grazie and its annexes are to be found to the northwest of the intersection of Kolyva Street and Kolokotroni Street, partly below the asphalt and partly under private property of emergency lodgings, which date from the ’53 earthquake, and partly under a fairly new construction.
To enrich the GIS of the first phase, a geophysical approach of anomalies under the surface should now follow. In this urban environment only non-destructive methods like ground penetrating radar (GPR) and electrical resistivity tomography (ERT) can be carried out. With the necessary permissions and funding, a team of researchers could be deployed to collect and process such data. If these are conclusive, a third phase of small scale excavations in search of remains may follow. To top up personal investments, Vesalius Continuum(9) has launched a crowd funding campaign to sponsor the second phase. If you wish to contribute to finding the real cause of Vesalius’s death and help Pascalle Pollier reconstruct the face of a genius whose legacy survives to this very day, visit: www.gofundme.com/VesaliusContinuum
Personal note: Click on the following link to collaborate with this incredible quest. I already did. Dr. Miranda
Notes and Sources:
(1) The author thanks Maurits Biesbrouck, Sylviane Déderix, Jan Driessen, Theodoor Goddeeris, Akis Ladikos, Pavlos Plessas, Pascale Pollier, Apostolos Sarris, Maria Sidirokastriti - Kontoni and Omer Steeno.
(2) Maurits Biesbrouck upgraded Dr. Harvey Cushing’s list of publications on Vesalius to more than 3000 records: http://www.andreasvesalius.be , accessed 8 January 2017.
(3) In 2007 a Canadian book collector bought Vesalius’ own copy of the 1555 edition of the Fabrica, heavily annotated in preparation of a never published third edition. In 2014 Vesalius’ own annotated copy of Institutiones by his teacher, J.G. von Andernach, came to light.
(4) DIRIX, Theo: Andreas Vesalius and his hoaxes, con variazioni, in: Vesalius, Journal of the International Society of the History of Medicine, Vol. XXII, nr. 1, June 2016, Special Issue, Proceedings of A Tribute to Andreas Vesalius, Padua, Italy - December 2015, pp. 103 - 111.
(5) The source is post-mortem gossip spread in January 1565 by the French diplomat, Hubertus Languetus, in a note of 24 lines opening with: “rumour has it”. See: BIESBROUCK, Maurits, Theodoor GODDEERIS, Omer STEENO. ‘Post Mortem’ Andreae Vesalii (1514-1564), Deel I. De laatste reis van Andreas Vesalius en de omstandigheden van zijn dood), in: A.Vesalius, nr. 3 september 2015, Alfagen, Leuven, pp 154-161.
(6) In total four letters have been discovered by José Baron Fernandez in the archives of Simancas, described and published since 1965
(7) BIESBROUCK, Maurits, Theodoor GODDEERIS, Omer STEENO. ‘Post Mortem’ Andreae Vesalii (1514-1564), Deel II. Het graf van Andreas Vesalius op Zakynthos, (vervolg en slot na Deel I in vorig nummer), in: A.Vesalius, nr. 4 december 2015, Alfagen, Leuven, pp 193-200.
(8) ibid
(9) Within the initial ad hoc organising committee of the Vesalius Continuum Conference in September 2014 in Zakynthos, medical artist Pascale Pollier and the author, then Consul at the Embassy of Belgium in Athens, formed the Search team. See: DIRIX, Theo, In Search of Andreas Vesalius, The Quest for the Lost Grave, LannooCampus, Leuven, 2014.
GoFundMe Campaign for the next stage of the project
- Details
This article is part of the series "A Moment in History" where we honor those who have contributed to the growth of medical knowledge in the areas of anatomy, medicine, surgery, and medical research.
This is the continuation of the article “The Ephraim McDowell House and Museum (1)”
The first room we visited from the foyer was the library. Antique furniture, elegant oil lamps and in wooden built-in-the-wall shelfs an incredible collection of antique books from the 1700-1900’s covering everything from medicine and surgery to history, philosophy and poetry. One of the shelves pictured here had mostly medical books.
As a book collector I was so tempted to touch, open, and read some of the books, but they are only for display. I could recognize some of the books as items that I would like to own and place in my library. The docent explained that, as the custom of the times, the library was the place for men to meet, smoke, read, share a bourbon, and discuss the events and politics of the day.
The next room was the music room. Dr. McDowell played the violin while his wife played the piano, both on display as well as other antique instruments donated to the museum. Antique furniture and over the fireplace mantle two whale oil lamps. There are family portraits all over the house. One can almost imagine the life of the times…
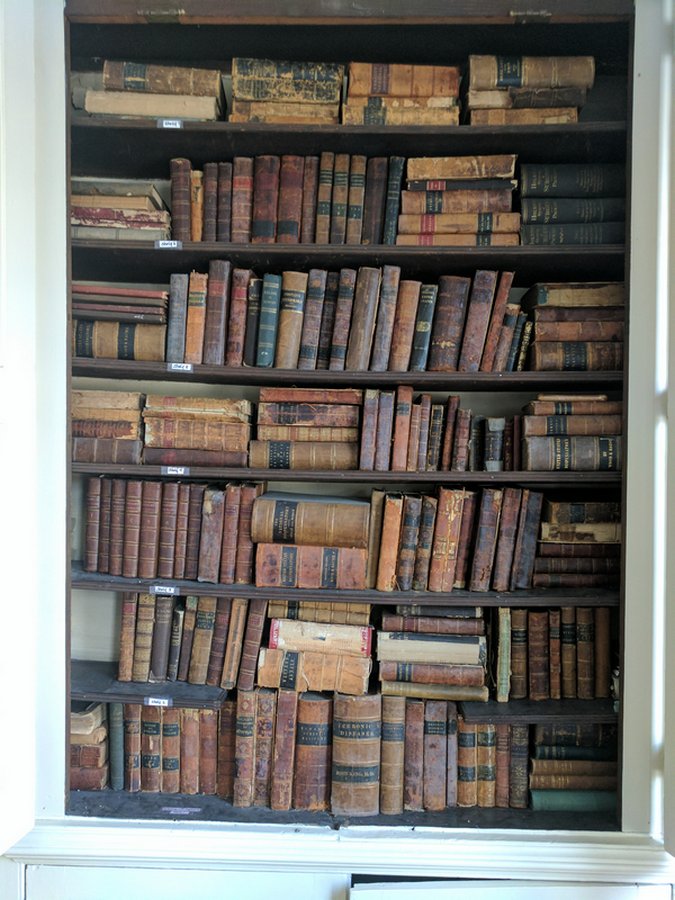 One of the library book shelves
One of the library book shelves
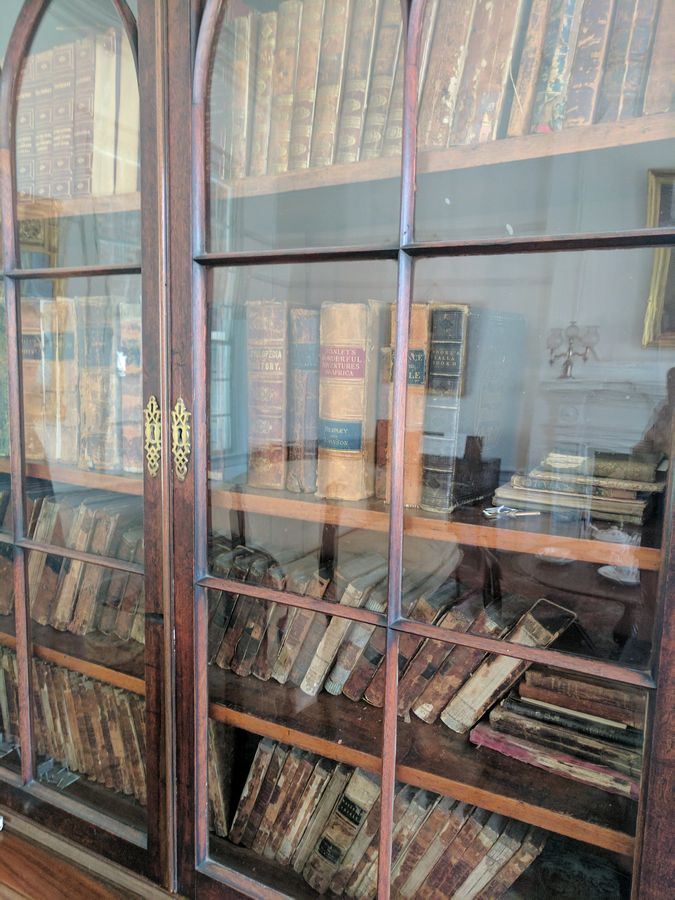 More books in the music room
More books in the music room

The music room
Interestingly, there is a large wooden door that opens from the foyer to the patio. The guide explained that it was a “casket door” so that people who died in the house could be taken through the door to the back of the house and not through the front door.
A wooden staircase leads to the second floor, where there is a small bedroom that was for the children. Because of the number of children, they had to sleep two or three to a bed. There is furniture, antique bedspreads, bedpans (there were no bathrooms in the house), even some toys, dolls, and chalk tablets.

The kids room

The master bedroom
The master bedroom is also on the second floor. Larger and more spacious, it was the place where women would get together to talk, knit and quilt. On the mantelpiece there is a family sword.
The next room is the “operating room” where history was made on Christmas Day, 1809.
- Details
This article is part of the series "A Moment in History" where we honor those who have contributed to the growth of medical knowledge in the areas of anatomy, medicine, surgery, and medical research.
In 2013 I wrote a short biography of Dr. Ephraim McDowell (1771- 1830) for the sidebar on this blog entitled “A Moment in History”. While researching the life of this illustrious surgeon I learned that his house is now a National Historic Landmark and has been transformed into a museum in the city of Danville, Kentucky. It took me almost four years but on Sunday February 19, 2017 I was able to go visit this place. Following is a series of articles and pictures of this visit.
The house itself was built in the 1790’s and most of it has been restored and lovingly maintained by the city, the Kentucky Medical Association, a Board of Directors, and a group of volunteers that work as docents giving tours of the house.
 The Ephraim McDowell House and Museum
The Ephraim McDowell House and Museum
 Dr. Miranda in front of the Ephraim McDowell House
Dr. Miranda in front of the Ephraim McDowell House
The following is an edited excerpt of Wikipedia on the McDowell House:
“After McDowell's death in 1830 the house was sold. It was the home of a Centre College president for a short time. Later the entire area became a slum and tenement property. The house deteriorated badly. Dr. August Schachner, of Louisville, led the efforts to buy the house for restoration. In 1921 he visited the house. "Since our last visit, the house has continued its downward course until it has reached a point where it now seems almost beyond redemption”. The room in the rear of the corresponding front room on the second floor,"(the operating room) "which is on a lower level by several feet, is used as a dump for the ashes from the grates of the rooms on the second floor."
The Kentucky Medical Association bought the house in 1935 and deeded it to the state of Kentucky, who had it restored by the Works Progress Administration (WPA). It was dedicated on May 20, 1939. In 1948, Kentucky returned the property to the Kentucky Medical Association.
The Kentucky Pharmaceutical Society restored the Apothecary Shop in the late 1950s with help from the Eli Lily Foundation. It was furnished by the Pfizer Laboratories. It was dedicated and presented to the Kentucky Medical Association on August 14, 1959.”
The house is located at 125 South Second Street, Danville, KY 40422. It is a white two-story wooden structure considered to be large for the time. To the right side stands a small one-story brick structure, the apothecary, where Dr. McDowell would provide medicine for his patients and others. To the left is the patio and garden where Dr. McDowell would grow medicinal plants for the apothecary. On the garden front there is a large two-sided plaque that reads:
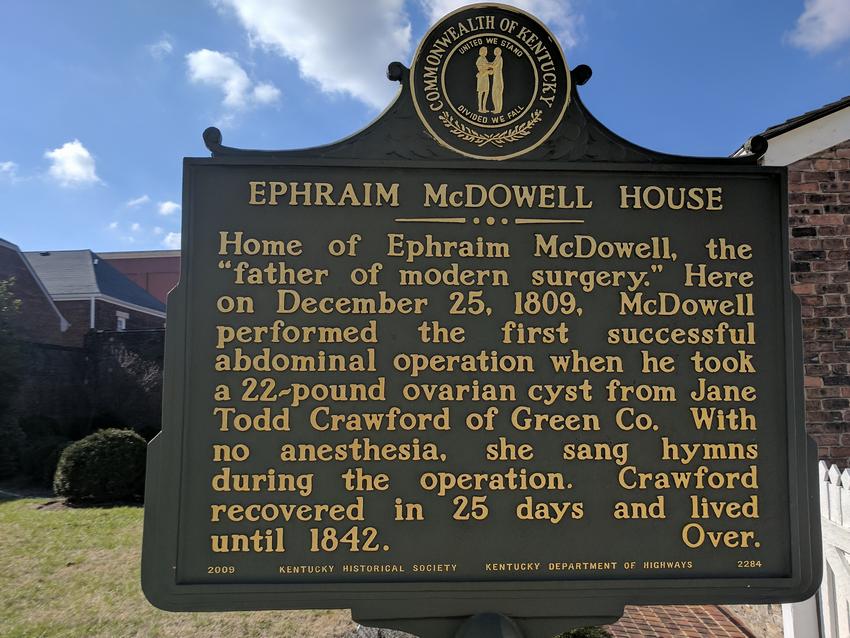
Front of the plaque at the Ephraim McDowell House
“Home of Ephraim McDowell, the “father of modern surgery.” Here on December 25, 1809 McDowell performed the first successful abdominal operation when he took a 22-pound ovarian cysts from Jane Todd Crawford of Green Co. With no anesthesia, she sang hymns during the operation. Crawford recovered in 25 days and lived until 1842”
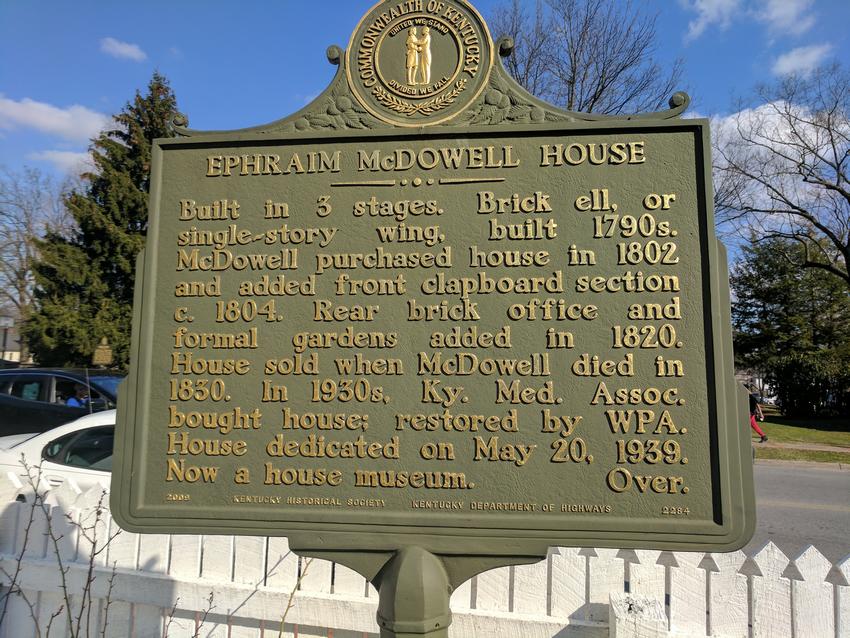
Back of the plaque at the Ephraim McDowell House
“Built in three stages. Brick ell, or single-story wing, built 1790s. McDowell purchased house in 1802 and added front clapboard section c.1804. Rear brick office and formal gardens added in 1820. House sold when McDowell dies in 1830. 1n 1930s, Ky. Med. Assoc. bought house; restored by WPA. House dedicated on May 20, 1939. Now a house museum”
- Details
This is a series of articles on depression published as a community service. The information in these articles follow our Privacy and Security Guidelines and cannot be construed as medical guidance. For additional information and counseling, consult with your physician or the appropriate health care professional of your choice. You can also find information on Transcranial Magnetic Stimulation (TMS) here. For the initial article on this series click here.
This article could also be entitled:
What is the difference between unipolar and bipolar depression?

Click for a larger image
Mood is a range of emotions that describe how we "feel" at a particular point in time. Mood is called a "visceral" (gut-like) sensation and is difficult to describe. It is a sensation dependent on a group of deep brain structures known as the limbic system.
Being a spectrum, there are two ends or "poles" to the range. An one end we have the major depressive mood of darkness, despair, and loathing of one's self. At the other end or "pole" we have the manic feeling of happiness, feeling "high", with extreme irritability and quick actions without measuring potential consequences.
An MDD patient that is "stuck" at the dark end of the spectrum, is said to be "unipolar", as the Latin word unus and uni- mean "one". The patient is always at one pole, therefore "unipolar".
Some depression patients have mood swings going from one end of the mood spectrum to the other. Since the medical prefix [bi-] means "two", these patients are said to have a "bipolar" type depression.
Some authors comment that there is not really a true unipolar depression for even unipolar depression patients move within the mood spectrum as their pathology evolves with treatment.
Experience tells us that as a depression patient starts to come out of their neurologically depressed state they may begin to show anxiety. This is easily treated by adding a secondary prescription course of right-sided low frequency treatment of TMS. As you go through your TMS Therapy treatment you may expect your prescription and dosage to change to accommodate your development towards a life without depression
References:
1. Barbee, J. G. (1998). Mixed symptoms and syndromes of anxiety and depression: Diagnostic, prognostic, and etiologic issues. Annals of Clinical Psychiatry, 10:15–29.
2. Regier, D. A., Rae, D. S., Narrow, W. E., Kaelber, C. T., & Schatzberg, A. F. (1998). Prevalence of anxiety disorders and their comorbidity with mood and addictive disorders. British Journal of Psychiatry. Supplement, 34: 24–28.
- Details
This is a series of articles on depression and published as a community service. The information in these articles follow our Privacy and Security Guidelines and cannot be construed as medical guidance. For additional information and counseling, consult with your physician or the appropriate health care professional of your choice. You can also find information on Transcranial Magnetic Stimulation (TMS) here. For the initial article on this series click here.
Medication
SSRIs and SNRIs
Tricyclics
MAOIs
FDA warning on antidepressants
Psychotherapy
Electroconvulsive therapy
Transcranial magnetic stimulation
The most common treatments for depression are medication and psychotherapy. Drugs are used to treat the primary disorder, but they can be strengthened with augmentation medication. Some patients take so many different medicines that they refer to them as their daily "cocktail". By their own nature drugs are unspecific in that they alter and influence the whole body. Depression drugs have a number of side effects. The side effects of some drugs is a listing of potentially dangerous events, as can be seen in this video.
To illustrate the side effects, following is a list of the side effects listed in the packaging of one of these modern less-side-effect drugs as listed by the manufacturer:
• Symptoms of aggression
• Irritability
• Panic attacks
• Extreme worry
• Restlessness
• Acting without thinking
• Abnormal excitement
• Thoughts of suicide
• If present, glaucoma symptoms may worsen
• May cause liver damage, and may not be taken if the patient has liver disease
• Alcohol consumption may increase some serious side effects
• The patient may feel drowsy
• May cause high blood pressure, dizziness, or lightheadedness

Click for a larger image
Medication
Antidepressants primarily work on brain neurotransmitters, especially serotonin and norepinephrine. Other antidepressants work on the neurotransmitter dopamine. Scientists have found that these particular chemicals are involved in regulating mood, but they are unsure of the exact ways that they work.
SSRIs and SNRIs
Some of the newest antidepressants are called selective serotonin reuptake inhibitors (SSRIs). Fluoxetine (Prozac), sertraline (Zoloft), escitalopram (Lexapro), paroxetine (Paxil), and citalopram (Celexa) are some of the most commonly prescribed SSRIs for depression. Serotonin and norepinephrine reuptake inhibitors (SNRIs) are similar to SSRIs and include venlafaxine (Effexor) and duloxetine (Cymbalta).
SSRIs and SNRIs tend to have fewer side effects than older antidepressants, but they do sometimes produce headaches, nausea, jitters, or insomnia when people first start to take them. These symptoms tend to fade with time. Some people also experience sexual problems with SSRIs or SNRIs, which may be helped by adjusting the dosage or switching to another medication.
One popular antidepressant that works on dopamine is bupropion (Wellbutrin). Bupropion tends to have similar side effects as SSRIs and SNRIs, but it is less likely to cause sexual side effects. However, it can increase a person's risk for seizures.
Tricyclics
Tricyclics are older antidepressants. Tricyclics are powerful, but they are not used as much today because their potential side effects are more serious. They may affect the heart in people with heart conditions. They sometimes cause dizziness, especially in older adults. They also may cause drowsiness, dry mouth, and weight gain. These side effects can usually be corrected by changing the dosage or switching to another medication. However, tricyclics may be especially dangerous if taken in overdose. Tricyclics include imipramine and nortriptyline.
MAOIs
Monoamine oxidase inhibitors (MAOIs) are the oldest class of antidepressant medications. They can be especially effective in cases of "atypical" depression, such as when a person experiences increased appetite and the need for more sleep rather than decreased appetite and sleep. They also may help with anxiety, panic attacks, and other specific symptoms.
However, people who take MAOIs must avoid certain foods and beverages (including cheese and red wine) that contain a substance called tyramine. Certain medications, including some types of birth control pills, prescription pain relievers, cold and allergy medications, and herbal supplements, also should be avoided while taking an MAOI. These substances can interact with MAOIs to cause dangerous increases in blood pressure. The development of a new MAOI skin patch may help reduce these risks.
MAOIs can also react with SSRIs to produce a serious condition called "serotonin syndrome," which can cause confusion, hallucinations, increased sweating, muscle stiffness, seizures, changes in blood pressure or heart rhythm, and other potentially life-threatening conditions. MAOIs should not be taken with SSRIs.
Sometimes stimulants, anti-anxiety medications, or other medications are used together with an antidepressant, especially if a person has a co-existing illness. However, neither anti-anxiety medications nor stimulants are effective against depression when taken alone, and both should be taken only under a doctor's close supervision.
FDA warning on antidepressants
Despite the relative safety and popularity of SSRIs and other antidepressants, studies have suggested that they may have unintentional effects on some people, especially adolescents and young adults. In 2004, the Food and Drug Administration (FDA) conducted a thorough review of published and unpublished controlled clinical trials of antidepressants that involved nearly 4,400 children and adolescents. The review revealed that 4 percent of those taking antidepressants thought about or attempted suicide (although no suicides occurred), compared to 2 percent of those receiving placebos.
This information prompted the FDA, in 2005, to adopt a "black box" warning label on all antidepressant medications to alert the public about the potential increased risk of suicidal thinking or attempts in children and adolescents taking antidepressants. In 2007, the FDA proposed that makers of all antidepressant medications extend the warning to include young adults up through age 24. A "black box" warning is the most serious type of warning on prescription drug labeling.
The warning emphasizes that patients of all ages taking antidepressants should be closely monitored, especially during the initial weeks of treatment. Possible side effects to look for are worsening depression, suicidal thinking or behavior, or any unusual changes in behavior such as sleeplessness, agitation, or withdrawal from normal social situations. The warning adds that families and caregivers should also be told of the need for close monitoring and report any changes to the doctor. The latest information from the FDA can be found on their website.
Results of a comprehensive review of pediatric trials conducted between 1988 and 2006 suggested that the benefits of antidepressant medications likely outweigh their risks to children and adolescents with major depression and anxiety disorders.
Psychotherapy
Two main types of psychotherapies—cognitive-behavioral therapy (CBT) and interpersonal therapy (IPT)—are effective in treating depression. CBT helps people with depression restructure negative thought patterns. Doing so helps people interpret their environment and interactions with others in a positive and realistic way. It may also help you recognize things that may be contributing to the depression and help you change behaviors that may be making the depression worse. IPT helps people understand and work through troubled relationships that may cause their depression or make it worse.
For mild to moderate depression, psychotherapy may be the best option. However, for severe depression or for certain people, psychotherapy may not be enough. For example, for teens, a combination of medication and psychotherapy may be the most effective approach to treating major depression and reducing the chances of it coming back. Another study looking at depression treatment among older adults found that people who responded to initial treatment of medication and IPT were less likely to have recurring depression if they continued their combination treatment for at least 2 years.
Electroconvulsive therapy
For cases in which medication and/or psychotherapy does not help relieve a person's treatment-resistant depression, electroconvulsive therapy (ECT) may be useful. ECT, formerly known as "shock therapy," once had a bad reputation. But in recent years, it has greatly improved and can provide relief for people with severe depression who have not been able to feel better with other treatments.
Before ECT begins, a patient is put under brief anesthesia and given a muscle relaxant. He or she sleeps through the treatment and does not consciously feel the electrical impulses. Within 1 hour after the treatment session, which takes only a few minutes, the patient is awake and alert.
A person typically will undergo ECT several times a week, and often will need to take an antidepressant or other medication along with the ECT treatments. Although some people will need only a few courses of ECT, others may need maintenance ECT—usually once a week at first, then gradually decreasing to monthly treatments.
ECT may cause some side effects, including confusion, disorientation, and memory loss. Usually these side effects are short-term, but sometimes they can linger. Newer methods of administering the treatment have reduced the memory loss and other cognitive difficulties associated with ECT.
FDA cleared in 2008, Transcranial Magnetic Stimulation (TMS) is one of the most promising therapies in the arsenal against depression. One of the key advantages of TMS is that while medical treatment is generalized, affecting the whole body, TMS targets the area of the brain most related in cortical control of mood changes, the left dorsolateral prefrontal cortex. With minimal and very localized side effects, repetitive TMS (rTMS) treatment has proven very effective.
Next: Depression and anxiety