![]()
Medical Terminology Daily (MTD) is a blog sponsored by Clinical Anatomy Associates, Inc. as a service to the medical community. We post anatomical, medical or surgical terms, their meaning and usage, as well as biographical notes on anatomists, surgeons, and researchers through the ages. Be warned that some of the images used depict human anatomical specimens.
You are welcome to submit questions and suggestions using our "Contact Us" form. The information on this blog follows the terms on our "Privacy and Security Statement" and cannot be construed as medical guidance or instructions for treatment.
We have 357 guests and no members online
")
Marcia Crocker Noyes
(1869 – 1946)
Further to my comment on old books and research that started with an interesting bookplate (Ex-Libris). I continued my research and found that the person in charge of the Osler library bookplate was a fascinating individual that today maybe a ghost in the MedChi library and building in Baltimore... This is certainly an article that can be called "A Moment in History"
Marcia Crocker Noyes was the librarian at The Maryland State Medical Society from 1896 to 1946 and was a founding member of the Medical Library Association.[1][2][3]
Sir William Osler, MD. a famous Johns Hopkins surgeon was a noted bibliophile and had a large personal collection of books on various topics. When he became the President of MedChi in 1896, he was dismayed at the condition of the library and knew that with the right person and some stewardship, it could become a significant collection. Sir William asked his friend, Dr. Bernard Steiner, a physician and President of the Enoch Pratt Free Library in Baltimore for suggestions of a librarian, and Dr. Steiner recommended Marcia Crocker Noyes. A native of New York, and a graduate of Hunter College, Marcia had moved to Baltimore for a lengthy visit with her sister, and took a “temporary” position at the Pratt Library, which turned into three years. Although she had no medical experience or background, she was enthusiastic, and most importantly, she was willing to move into the apartment provided for the librarian, who needed to be available 24 hours a day.
The image in this article is Ms. Noyes on her first year on the job. Marcia developed a book classification system for medical books, based on the Index Medicus, and called it the Classification for Medical Literature. The system uses the alphabet with capital letters for the major divisions of medicine and lower-case ones for the sub-sections. The system was used for many years, but it's now dated and the Faculty's original shelving scheme was never changed. The card catalogs still reflect her classification and many of the cards are written in Marcia's back-slanting handwriting.
Marcia knew enough to ask the Faculty's members about medical questions, terminology and literature. She gradually won over the predominantly male membership and they became her greatest allies; Sir William at the start, and then for nearly 40 years, Dr. John Ruhräh, a wealthy pediatrician with no immediate family of his own. She made a point of attending almost every Faculty function, and in 1904, under guidelines from the American Medical Association, Marcia was made the Faculty Secretary. For much of her first 10 years, she was the Faculty's only full-time employee, only being assisted by Mr. Caution, the Faculty's janitor. Later in life Marcia would say that she hired him because of his name!
Within ten years, the library had outgrown its space, and plans, spearheaded by Marcia and Sir William before his move to Oxford, were made to build a headquarters building, mainly to house the library's growing collection of medical books and journals.
Marcia was instrumental in the design and building of the new headquarters. She travelled to Philadelphia, New York and Boston to look at their medical society buildings, and eventually, the Philadelphia architectural firm, Ellicott & Emmart was selected to design and build the new Faculty building. Every detail of the building held her imprimatur, from the graceful staircase, to the light-filled reading room, and all of the myriad details of the millwork, marble tesserae, and most of all, the four-story cast iron stacks. She was on-site, climbing up unfinished staircases, checking out the progress of the building, which was built in less than one year at a cost of $90,000.
Among the features of the new building was a fourth-floor apartment for her. She referred to it as the "first penthouse in Baltimore" and it had a garden and rooftop terrace. The library collection eventually grew to more than 65,000 volumes from medical and specialty societies around the world. Journals were traded back and forth, and physicians eagerly anticipated the arrival of each new issue. At the same time, Marcia was involved in the Medical Library Association as one of eight founding members. The MLA promotes medical libraries and the exchange of information. One of the earliest mandates of the MLA was the Exchange, a distribution and trade service for those who had duplicates or little-used books in their collections. Initially, the Exchange was run out of the Philadelphia medical society, but in 1900 it was moved to Baltimore and Marcia oversaw it. Several hundred periodicals and journals were received and sent each month, a huge amount of work for a tiny staff. In 1904, the Faculty had run out of room to manage the Exchange, so it was moved to the Medical Society of the Kings County (Brooklyn). But without Marcia's excellent administrative skills, it floundered and in 1908, the MLA asked Marcia to take charge once again.
In 1909, when the new Faculty building opened, there was enough room to run the Exchange and with the help of MLA Treasurer, noted bibliophile and close friend, Dr. John Ruhräh, it once again became successful. Additionally, Marcia and Dr. Ruhräh combined forces to revive the MLA's bulletin, which had all but ceased publication in 1908, taking the Exchange with it. This duo maintained editorial control from 1911 until 1926. In 1934, around the time of Dr. Ruhräh's death, Marcia became the first “unmedicated” professional to head the MLA. During her tenure, the MLA incorporated, the first seal was adopted, and the annual meeting was held in Baltimore. Marcia wanted to write the history of the MLA once she retired from full-time work at the Faculty, but her health was beginning to fail. She had back problems and had suffered a serious burn on her shoulder as a young woman, possibly from her time running a summer camp, Camp Seyon, for young ladies in the Adirondack Mountains. In 1946, a celebration was planned to honor Marcia's 50 years at the Faculty. But she was adamant that the physicians wait until November, the actual date of her 50 years. However, they knew she was gravely ill, and might not make it until then, so a huge party was held in April. More than 250 physicians attended the celebration, but the ones she was closest to in the early years, were long gone. She was presented with a suitcase, a sum of money to use for travelling, and her favorite painting of Dr. John Philip Smith, a founder of the Medical College in Winchester, Virginia. It was painted by Edward Caledon Smith, a Virginia painter who had been a student of the painter Thomas Sully.[4] She adored this painting and vowed, jokingly, to take it with her wherever she went.
The painting was not to stay with her for very long, for she died in November 1946, and left it to the Faculty in her will. Her funeral was held in the Faculty's Osler Hall, named for her dear friend. More than 60 physicians served as her pallbearers, and she was buried at Baltimore's Green Mount Cemetery. In 1948, the MLA decided to establish an award in the name of Marcia Crocker Noyes. It was for outstanding achievement in medical library field and was to be awarded every two years, or when a truly worthy candidate was submitted. In 2014, the Faculty began giving a bouquet of flowers to the winner of the award in Marcia's name, and in honor of her work. Much evidence exists for this tradition, as we know that the physicians, especially Drs. Osler and Ruhräh, frequently gave her bouquets of flowers. Marcia also cultivated flower gardens at the Faculty and decorated the rooms with her work.
Today, the MedChi building is open for tours and if the rumors are to be believed Ms. Marcia Crocker Noyes is still at work in her beloved library as the "resident ghost" [1][5]

NOTE: This article has been modified from the original Wikipedia article on Marcia Crocker Noyes. The article itself is well-written with interesting images of the subject. I would encourage you to visit it. The second insert is from book 00736 in my personal library and shows in pencil, the incredibly small handwriting of Marsha C. Noyes.
Sources:
1. "Marcia, Marcia, Marcia" MedChi Archives blog.
2. "Marcia C. Noyes, Medical Librarian" (PDF). Bulletin of the Medical Library Association. 35 (1): 108–109. 1947. PMC 194645
3. Smith, Bernie Todd (1974). "Marcia Crocker Noyes, Medical Librarian: The Shaping of a Career" (PDF). Bulletin of the Medical Library Association. 62 (3): 314–324. PMC 198800Freely accessible. PMID 4619344.
4. Edward Caledon BRUCE (1825-1901)"
5. Behind the scenes tour MedChiBuilding
"Clinical Anatomy Associates, Inc., and the contributors of "Medical Terminology Daily" wish to thank all individuals who donate their bodies and tissues for the advancement of education and research”.
Click here for more information
- Details
- Written by: Fernanda Cortes, DDS, MSc
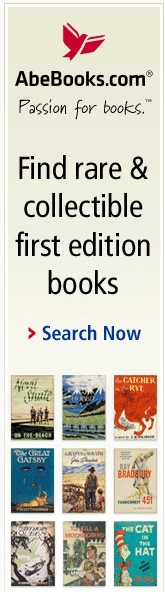
Figure A: Incomplete PP viewed from the
posterior aspect of the articular fossa
related to the retroglenoid tubercle
The Ponticulus Posticus (PP), also known as the pons arcuatus, foramen arcuale, and arcuate foramen, is a bony bridge that connects the retroglenoid tubercle with the posterior arch of the C1 vertebra, also known as the Atlas.
It substitutes the lateral segment of the posterior atlantooccipital ligament or joint capsule (1) on the area which stabilizes the vertebral artery on its emergency of the transverse foramen of the Atlas (2). This bridge or arch could be thick, thin or even incomplete (2). The importance of this calcification relies on the fact that it has been linked with cervicogenic headache (1,3) chronic tension-type headaches, sensorineural hearing loss (4), shoulder and arm pain, neck pain, and vertigo (1, 5).
The presence of a ponticulus posticus could also impact the planning of high cervical surgeries associated with the Atlas [C1] (6). A recent meta-analysis of the prevalence of this condition worldwide found an overall prevalence of a complete PP of 9.1% versus an incomplete PP, which was 13.6%. In males (10.4%) the complete PP was more common than in females (7.3%), but an incomplete PP was more commonly seen in females (18.5%) than in males (16.7%) (7).

Figure B: Complete PP. It crosses from the
retroglenoid tubercle down to the
posterior arch.
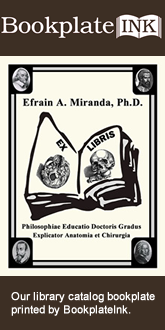
Despite the fact that this calcification has been associated with different painful disorders, some other authors consider it an anatomical condition destined to protect the vertebral artery and not a pathological condition (8). PP is visible on lateral cervical spine and cranial lateral radiographs as thin bony arch on the shape of a ring crossing from the retroglenoid tubercle to the posterior arch of C1, being either partially of fully calcified (Figures C and D).
Note 1: For the etymology of the term glenoid, click here.
Note 2: Figures C and D can be found at the bottom of the article
Sources:
1. Ross JS, Moore KR, editors. Diagnostic Imaging: Spine E-Book. 3rd ed. Philadeplphia: Elsevier; 2015. 31 p.
2. Torres Cueco R. La Columna Cervical: Evaluación Clínica y Aproximaciones Terapéuticas. Principios anatómicos, funcionales, exploración clínica y técnicas de tratamiento. Tomo I. 1° Ed. Madrid: Medica Panamericana; 2008. 124 p.
3. Tambawala SS, Karjodkar FR, Sansare K, Motghare D, Mishra I, Gaikwad S, Dora AC. Prevalence of Ponticulus Posticus on Lateral Cephalometric Radiographs, its Association with Cervicogenic Headache and a Review of Literature. World Neurosurg [Internet]. 2017 Apr 17(cited 02 Jun 2017). pii: S1878-8750(17)30525-9. Available at: doi: 10.1016/j.wneu.2017.04.030. [Epub ahead of print]
4. Koutsouraki E, Avdelidi E, Michmizos D, Kapsali SE, Costa V, Baloyannis S. Kimmerle's anomaly as a possible causative factor of chronic tension-type headaches and neurosensory hearing loss: Case report and literature review. Int J Neurosci. 2010; 120:236-9
5. Cakmak O, Gurdal E, Ekinci G, Yildiz E, Cavdar S. Arcuate foramen and its clinical significance. Saudi Med J. 2005; 26:1409-13.
6. Song MS, Lee HJ, Kim JT, Kim JH, Hong JT. Ponticulus posticus: Morphometric analysis and Its anatomical Implications for occipito-cervical fusion. Clin Neurol Neurosurg [Internet]. 2017 Jun (cited 02 Jun 2017);157:76-81. Available at: doi: 10.1016/j.clineuro.2017.04.001. Epub 2017 Apr 3.
7. Pękala PA, Henry BM, Pękala JR, Hsieh WC, Vikse J, Sanna B, Walocha JA, Tubbs RS, Tomaszewski KA. Prevalence of foramen arcuale and its clinical significance: a meta-analysis of 55,985 subjects. J Neurosurg Spine [Internet]. 2017 Jun (cited 02 Jun 2017); 16:1-15. Available at: doi: 10.3171/2017.1.SPINE161092. [Epub ahead of print]
8. Schilling J, Schilling A, Suazo I. Ponticulus posticus on the Posterior Arch of Atlas, Prevalence Analysis in Asymptomatic PatientsInt. J. Morphol. 2010 Mar; 28(1):317-322.
Acknowledgments: The Atlas [C1] specimens shown on figures A and B belong to the Anatomy department of the Medical College of the Finis Terrae University, Santiago, Chile and are used to show two examples of PP. With permission.
Article written by Prof. M. Fernanda Cortes, DDS, MsC.
 Figure C: Complete PP shown on a lateral radiographic view. Figure D: Partial PP shown on a lateral radiographic view.
Figure C: Complete PP shown on a lateral radiographic view. Figure D: Partial PP shown on a lateral radiographic view.
- Details

Wax bust of Andreas Vesalius by Pascale Pollier
Friends of Medical Terminology Daily:
As you know, we are part of an incredible quest to find the body of Andreas Vesalius, recognized worldwide as the Father of Modern Anatomy. His life and the story and legends about his death are part now of scientific fact and folklore.
The quest for the lost grave of Andreas Vesalius has been published in this blog several times. Many of the members of this group, such as Pascale Pollier, Theo Dirix, Dr. Sylvianne Déderix, Dr. Maurits Biesbrouck, etc. are contributors to Medical Terminology Daily.
The project has had several stages and you are welcome to follow the above links to the authors to read their contributions which clarify the scope and objectives of this quest, including Theo Dirix's article : "To put it in another way: where do we have to look for Vesalius's grave?".
The project next step is to perform a detailed research on the area where we suspect (actually know with a high degree of certainty) where the cemetery of the Church of Santa Maria delle Grazie (Zakynthos, Greece) used to be.

Church of Santa Maria delle Grazie
The problem was to obtain the permits to do the non-invasive radar scan of the grounds in the area... and this is the exciting news! Following is the press release:
"The Belgian School of Archaeology)in Athens (EBSA) just obtained the permission for a new archaeological project at Zakynthos in collaboration with the local Ephorate and Dr Merkouri, as well as the IMS in Rethymnon (Dr A. Sarris). The project, initiated and coordinated by Theo Dirix and Pascale Pollier, concerns the quest for the tomb of the Belgian anatomist, father of modern anatomy, Andreas Vesalius who died and was buried in the island."
Needless to say, we are all excited. Now we have to fund this research, and you can all help by contributing as little or as much as you can to the GoFundMe page. We are very close to our objective and this will allow us to pay the permits, rent the equipment and finally get a little closer to finding Andreas Vesalius.
Personal note: Click on the following link to collaborate with this incredible quest. I already did. Dr. Miranda
GoFundMe Campaign for the next stage of the project
- Details
")
Arterial Circle of Willis
UPDATED: The arterial "circle of Willis" is a roundabout of arteries found at the base of the brain, allowing for collateral circulation at this level. This arterial circle has been described by many anatomists, but it was Thomas Willis (1621 - 1675) who described it in most detail, and he was the first to understand its function.
The circle of Willis receives blood from the two main paired arteries that provide blood supply to the head and brain: the carotid arteries anteriorly, and the vertebral arteries posteriorly.
This arterial circle is formed by the anastomosis of several arteries, paired and unpaired:
• Anterior cerebral arteries: These paired arteries are one of the terminal branches of the internal carotid arteries. They provide blood supply to the medial aspect and part of the lateral aspect of frontal and parietal lobes of the brain
• Anterior communicating artery: A single unpaired small artery communicating both anterior cerebral arteries and providing potential collateral circulation between them
• Internal carotid arteries: These two bilateral arteries are one of the branches of the carotid artery found at the root of the neck. Its two main terminal branches are the anterior cerebral arteries and the middle cerebral arteries.
• Posterior cerebral arteries: These two arteries are formed by the bifurcation of the basilar artery, which itself is formed by the junction of the right and left vertebral arteries. The posterior cerebral arteries provide blood supply to the occipital lobe and part of the temporal lobe of the brain
• Posterior communicating arteries: These paired arteries provide communication between the carotid and vertebral arterial territories
• Middle cerebral arteries: Although not technically part of the arterial circle of Willis, these paired arteries are one of the two terminal branches of the internal carotid arteries. The middle cerebral artery travels deep in the lateral sulcus (Sylvian fissure) of the brain and provides blood supply to the lateral aspect of the brain including the frontal, parietal, occipital, temporal, and insular lobes
The arterial circle of Willis provides all of the arterial blood to the brain. Cerebral blood flow in humans averages 55 mL per 100 g of brain tissue per minute. This is a about over 742.5 mL/min for the average 1350 g brain. Depending on the situation the brain will use between 15 to 20 percent of the total cardiac output, although by weight the brain is only about two to three percent of the average body weight. Incredibly, the brain uses more oxygen that most organs averaging close to 25% of the total oxygen needs of the body!
The importance of the arterial circle of Willis is that beyond this point the arterial supply to the brain becomes terminal, that is, there are little or no anastomoses between the bifurcating branches exposing the brain to ischemia and necrosis should there be an arterial stenosis or stricture. The circle of Willis is an area prone to aneurysms, with over 27,000 cases yearly in the US.
For an image of the vascular territories of the brain, click here.
{kind=link}
Thanks to Jackie Miranda-Klein for making me review this post and update it!... and congratulations to Jackie for starting her Physician Assistant Master's degree at Kettering College. Dr. Miranda.
Image in the Public Domain. Courtesy of www.wikipedia.org
Clinical anatomy, pathology, and surgery of the brain and spinal cord are some of the lecture topics developed and delivered by Clinical Anatomy Associates, Inc.
- Details
- Written by: Fernanda Cortes, DDS, MSc
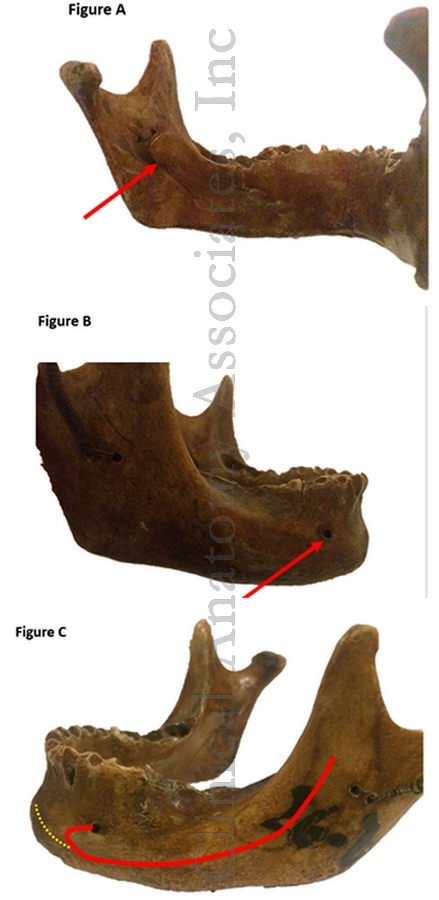
Click for a larger image
The mandibular canal is a long, bilateral canal which runs along and within the mandible. This canal transports the inferior alveolar neurovascular bundle. The mandible is known vernacularly as the “jawbone” or “lower jaw”.
The mandibular canal starts on the medial surface of the mandibular ramus at the mandibular foramen (Figure A, arrow) descends anteroinferiorly through the body of the mandible until it ends in the mental foramen at the buccal (anterior) surface of the mandible, usually in the area between the premolars (Figure B, arrow).
Before exiting, the canal forms an “anterior loop” projected anterior to the mental foramen prior to changing its direction back and outwards in direction to the buccal plate (Figure C, red line). This last portion of the canal is called the “mental canal”.
A frequent anatomical variation is the presence of a bifid mandibular canal (recent studies indicate it has a prevalence of around 16%).
Different anatomical studies show that the mandibular canal not only finishes at the mental foramen, but it could divide itself giving an incisive canal which runs anteriorly onto the incisal region (Figure C, yellow line). When it doesn’t continue as an incisal canal, the neurovascular elements go anteriorly through the cells of the spongy bone tissue.
The presence of this Incisal canal has surgical relevance, and knowledge of its exact location and anatomical parameters has a high importance on reducing complications of surgical procedures in the mental area such as dental implants, bone lesions removal and bone harvesting among others, all which could damage the incisal canal and the neurovascular bundle inside it.
With the latest use of CBCT (Cone Beam Computed Tomography) technology to evaluate anatomical structures, the presence of this canal has showed to be high (92-100%) and its length can vary from reaching only the premolar area or even the central mandibular incisors in the least of cases.
Sources:
1. Haas LF, Dutra K, Porporatti AL, Mezzomo LA, De Luca Canto G, Flores-Mir C, Corrêa M. Anatomical variations of mandibular canal detected by panoramic radiography and CT: a systematic review and meta-analysis. Dentomaxillofac Radiol. 2016;45(2):20150310.
2. Kong N, Hui M, Miao F, Yuan H, Du Y, Chen N. Mandibular incisive canal in Han Chinese using cone beam computed tomography. Surg Radiol Anat. 2016 Nov 11. [Epub ahead of print] Int J Oral Maxillofac Surg. 2016 Sep;45(9):1142-6.
3. Rouvierre H, Delmas A. Anatomía humana: Descriptiva, topográfica y funcional. Cabeza y cuello. Volumen 1. 11° ed. España: Masson, S.A.;2005. P. 114.
4. Von Arx T, Lozanoff S. Clinical Oral Anatomy: A Comprehensive Review for Dental Practitioners and researchers. Switzerland: Springer; 2016. P 323- 390
Article and image provided by Prof. M. Fernanda Cortes, DDS, MsC.
- Details
- Written by: Efrain A. Miranda, Ph.D.
Lithopedion Clark,JG 1897
This word originates from the root terms [-lith-], which arises from the Greek word [λίθος] meaning “stone” and the term [-pedion-] (or [pædion]) which is also Greek [παιδί] meaning “child”. In simple terms this would mean a “stone child”.
Strangely enough, “stone children” or lithopædia are rare cases found in nature, and have been described in humans since early times, the first one by Abū al-Qāsim (Abulcasis) in the 10th century.
When found, it is usually a fetus of more than 12 weeks of estimated age. This is because a younger fetus, if it dies, will usually be reabsorbed by the mother’s body. Usually they are ectopic pregnancies where the fetus dies and is calcified, turning into “stone”.
Technically there are three types of lithopaedia:
1. Lithokelyphos: Only the surrounding fetal membranes calcify. The fetus decomposes and is absorbed, while the calcified membranes protect the mother from the effects of necrosis.
2. Lithokelyphopaedion: Where the membranes and the fetus calcify.
3. True lithopedion, also known as “lithopedion proper”, or lithotecnon. The most common presentation when found, only the fetus is calcified.
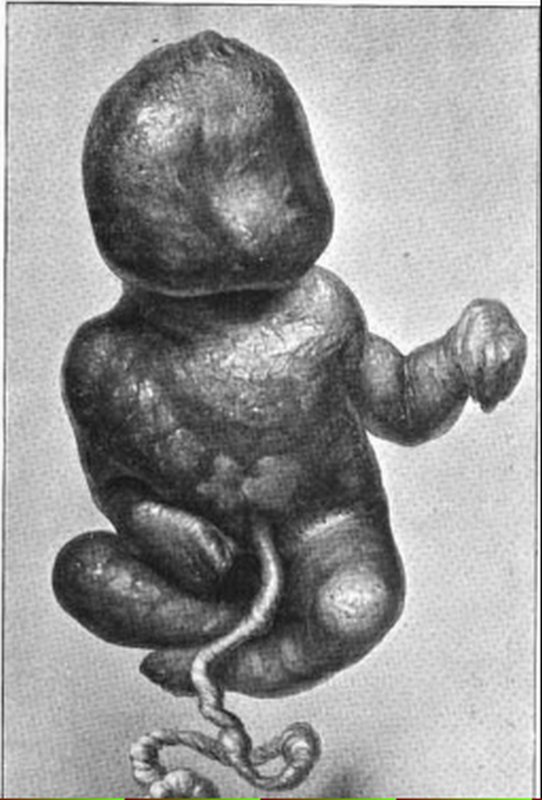
The incidence of lithopedia is estimated close to 1.8% of ectopic pregnancies. The following images are of a lithopedion case described by Bainbridge in 1911 and include an X-Ray of the lithopedion.
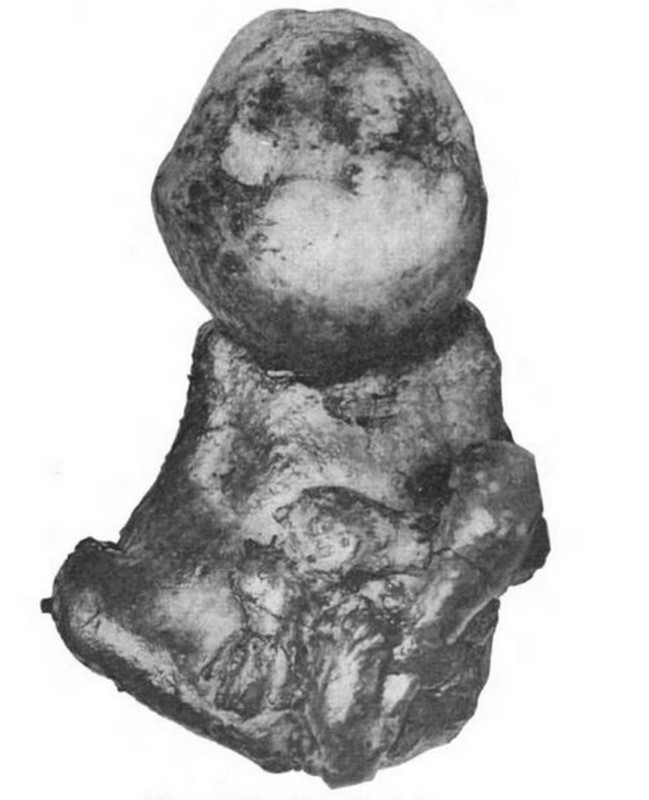
Lithopedion
Click for a larger image

Lithopedion
Click for a larger image
Sources:
1. “A rare case of Lithopedion” Clark, JG John Hopkins Hospital Bulletin Volume 8 (1897) 221-228
2. “Lithopedion, Report of a case with a review of the literature” Bainbridge, WS. Am J Obstr V65 (1911) 31 – 52
3. “Chilean woman carried calcified foetus for 50 years” BBC News
4. Blog: James Edwards Hughes “The Lithopedion”
- Details
This article is part of the series "A Moment in History" where we honor those who have contributed to the growth of medical knowledge in the areas of anatomy, medicine, surgery, and medical research.
This is the continuation of the article “The Ephraim McDowell House and Museum (3)”. For the first article, click here.
The rest of the house is interesting. The kitchen is an open hearth typical of the times and beneath the operating room. Candle molds, butter churners, baking tables, iron cooking utensils, etc. The guide explained that most of the cooking work was done by slaves.
To the back of the house if a large garden. Part of it is shaped as a Maltese cross, and this is where Dr. McDowell cultivated medicinal plants and herbs for his practice and the apothecary, The garden has several monuments, one of which is the original slab that covered Dr. McDowell's tomb.

The kitchen

The back of the house
The apothecary
This "pharmacy" of the times is incredibly well-preserved, maintained and furnished. It is said that Dr. McDowell worked so much at this place that he eventually moved to the country to a second house he named "Cambiskenneth" after a famous local native american chief.
The apothecary has a basement that is off-limits to visitors, but there are photographs of the location for visitors to see.
Some of the porcelain and glass containers still have some of their contents.

The apothecary

The apothecary
Additional historic buildings
Just across from the McDowell House and Museum is the Constitution Square, a site that I would encourage you to visit. Following is an excerpt of the Danville KY website on the Constitution Square Historic Site:
"This is the birthplace of Kentucky's statehood. In 1776, Kentucky was still part of the frontier and a county of Virginia. The Wilderness Road, blazed by Daniel Boone, led pioneers through the Cumberland Gap and into Central Kentucky. Danville's prominent location on the Wilderness Road caused it to become a crossroad for early settlers, and a center of political activity.
By 1785, Danville was chosen as Kentucky's first seat of government, and a meetinghouse, courthouse and jail were built to administer the growing territory. Still bound to Virginia laws, though, several Danville citizens formed the political club that recognized the need for a convention to discuss statehood. Between 1784-1792, ten constitutional conventions took place at the courthouse of Constitution Square. In 1790, Kentucky delegates accepted Virginia's terms for separation from the state. On June 1, 1792, Kentucky became the fifteenth state in the union, and Isaac Shelby, a Revolutionary War hero, was named the first Governor of the Commonwealth."
Several original buildings and replicas are found at this site.
In closing this series of articles I can only say that this was an interesting personal and learning experience. Being able to visit The Ephraim McDowell House and Museum allowed me to envision the life of this time. To place it in perspective the year that Dr. McDowell operated on Mrs. Crawford was 1809. On the same year Abraham Lincoln was born (only 35 miles from the farm of Mrs. Crawford), James Madison was the 4th president of the United States of America (which had only 15 states and 6 territories), Napoleon occupied Vienna, and Ludwig van Beethoven had just finished writing his Fifth Symphony.
Following is a large image of the original house prior to its renovation. The image is in the public domain from a biographical book by Dr. McDowell's granddaughter Mary Young Ridenbaugh.
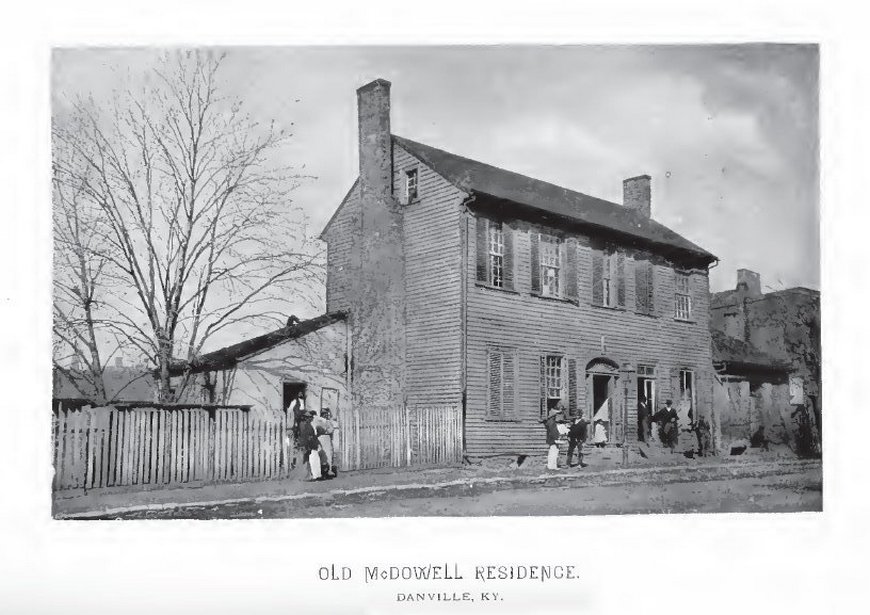
Click on the image for a larger depiction
Sources:
1. “Ephraim McDowell and Jane Todd Crawford, the Bicentennial of a Surgical Masterpiece” Benigno, BB Obst & Gynecol (2009) 113. 5:1141-1144
2. “The Biography of Ephraim McDowell, M.D.; The Father of Ovariotomy” Ridenbaugh, MY, 1890 CL Webster & Co.
3. “Ephraim McDowell: "Father of ovariotomy" and founder of abdominal surgery, with an appendix on Jane Todd Crawford” Schachner, A 1921, J.B. Lippincott Co. (Interesting discovery in an Ex-Libris in this book)