![]()
Medical Terminology Daily (MTD) is a blog sponsored by Clinical Anatomy Associates, Inc. as a service to the medical community. We post anatomical, medical or surgical terms, their meaning and usage, as well as biographical notes on anatomists, surgeons, and researchers through the ages. Be warned that some of the images used depict human anatomical specimens.
You are welcome to submit questions and suggestions using our "Contact Us" form. The information on this blog follows the terms on our "Privacy and Security Statement" and cannot be construed as medical guidance or instructions for treatment.
We have 1042 guests and no members online
")
Marcia Crocker Noyes
(1869 – 1946)
Further to my comment on old books and research that started with an interesting bookplate (Ex-Libris). I continued my research and found that the person in charge of the Osler library bookplate was a fascinating individual that today maybe a ghost in the MedChi library and building in Baltimore... This is certainly an article that can be called "A Moment in History"
Marcia Crocker Noyes was the librarian at The Maryland State Medical Society from 1896 to 1946 and was a founding member of the Medical Library Association.[1][2][3]
Sir William Osler, MD. a famous Johns Hopkins surgeon was a noted bibliophile and had a large personal collection of books on various topics. When he became the President of MedChi in 1896, he was dismayed at the condition of the library and knew that with the right person and some stewardship, it could become a significant collection. Sir William asked his friend, Dr. Bernard Steiner, a physician and President of the Enoch Pratt Free Library in Baltimore for suggestions of a librarian, and Dr. Steiner recommended Marcia Crocker Noyes. A native of New York, and a graduate of Hunter College, Marcia had moved to Baltimore for a lengthy visit with her sister, and took a “temporary” position at the Pratt Library, which turned into three years. Although she had no medical experience or background, she was enthusiastic, and most importantly, she was willing to move into the apartment provided for the librarian, who needed to be available 24 hours a day.
The image in this article is Ms. Noyes on her first year on the job. Marcia developed a book classification system for medical books, based on the Index Medicus, and called it the Classification for Medical Literature. The system uses the alphabet with capital letters for the major divisions of medicine and lower-case ones for the sub-sections. The system was used for many years, but it's now dated and the Faculty's original shelving scheme was never changed. The card catalogs still reflect her classification and many of the cards are written in Marcia's back-slanting handwriting.
Marcia knew enough to ask the Faculty's members about medical questions, terminology and literature. She gradually won over the predominantly male membership and they became her greatest allies; Sir William at the start, and then for nearly 40 years, Dr. John Ruhräh, a wealthy pediatrician with no immediate family of his own. She made a point of attending almost every Faculty function, and in 1904, under guidelines from the American Medical Association, Marcia was made the Faculty Secretary. For much of her first 10 years, she was the Faculty's only full-time employee, only being assisted by Mr. Caution, the Faculty's janitor. Later in life Marcia would say that she hired him because of his name!
Within ten years, the library had outgrown its space, and plans, spearheaded by Marcia and Sir William before his move to Oxford, were made to build a headquarters building, mainly to house the library's growing collection of medical books and journals.
Marcia was instrumental in the design and building of the new headquarters. She travelled to Philadelphia, New York and Boston to look at their medical society buildings, and eventually, the Philadelphia architectural firm, Ellicott & Emmart was selected to design and build the new Faculty building. Every detail of the building held her imprimatur, from the graceful staircase, to the light-filled reading room, and all of the myriad details of the millwork, marble tesserae, and most of all, the four-story cast iron stacks. She was on-site, climbing up unfinished staircases, checking out the progress of the building, which was built in less than one year at a cost of $90,000.
Among the features of the new building was a fourth-floor apartment for her. She referred to it as the "first penthouse in Baltimore" and it had a garden and rooftop terrace. The library collection eventually grew to more than 65,000 volumes from medical and specialty societies around the world. Journals were traded back and forth, and physicians eagerly anticipated the arrival of each new issue. At the same time, Marcia was involved in the Medical Library Association as one of eight founding members. The MLA promotes medical libraries and the exchange of information. One of the earliest mandates of the MLA was the Exchange, a distribution and trade service for those who had duplicates or little-used books in their collections. Initially, the Exchange was run out of the Philadelphia medical society, but in 1900 it was moved to Baltimore and Marcia oversaw it. Several hundred periodicals and journals were received and sent each month, a huge amount of work for a tiny staff. In 1904, the Faculty had run out of room to manage the Exchange, so it was moved to the Medical Society of the Kings County (Brooklyn). But without Marcia's excellent administrative skills, it floundered and in 1908, the MLA asked Marcia to take charge once again.
In 1909, when the new Faculty building opened, there was enough room to run the Exchange and with the help of MLA Treasurer, noted bibliophile and close friend, Dr. John Ruhräh, it once again became successful. Additionally, Marcia and Dr. Ruhräh combined forces to revive the MLA's bulletin, which had all but ceased publication in 1908, taking the Exchange with it. This duo maintained editorial control from 1911 until 1926. In 1934, around the time of Dr. Ruhräh's death, Marcia became the first “unmedicated” professional to head the MLA. During her tenure, the MLA incorporated, the first seal was adopted, and the annual meeting was held in Baltimore. Marcia wanted to write the history of the MLA once she retired from full-time work at the Faculty, but her health was beginning to fail. She had back problems and had suffered a serious burn on her shoulder as a young woman, possibly from her time running a summer camp, Camp Seyon, for young ladies in the Adirondack Mountains. In 1946, a celebration was planned to honor Marcia's 50 years at the Faculty. But she was adamant that the physicians wait until November, the actual date of her 50 years. However, they knew she was gravely ill, and might not make it until then, so a huge party was held in April. More than 250 physicians attended the celebration, but the ones she was closest to in the early years, were long gone. She was presented with a suitcase, a sum of money to use for travelling, and her favorite painting of Dr. John Philip Smith, a founder of the Medical College in Winchester, Virginia. It was painted by Edward Caledon Smith, a Virginia painter who had been a student of the painter Thomas Sully.[4] She adored this painting and vowed, jokingly, to take it with her wherever she went.
The painting was not to stay with her for very long, for she died in November 1946, and left it to the Faculty in her will. Her funeral was held in the Faculty's Osler Hall, named for her dear friend. More than 60 physicians served as her pallbearers, and she was buried at Baltimore's Green Mount Cemetery. In 1948, the MLA decided to establish an award in the name of Marcia Crocker Noyes. It was for outstanding achievement in medical library field and was to be awarded every two years, or when a truly worthy candidate was submitted. In 2014, the Faculty began giving a bouquet of flowers to the winner of the award in Marcia's name, and in honor of her work. Much evidence exists for this tradition, as we know that the physicians, especially Drs. Osler and Ruhräh, frequently gave her bouquets of flowers. Marcia also cultivated flower gardens at the Faculty and decorated the rooms with her work.
Today, the MedChi building is open for tours and if the rumors are to be believed Ms. Marcia Crocker Noyes is still at work in her beloved library as the "resident ghost" [1][5]

NOTE: This article has been modified from the original Wikipedia article on Marcia Crocker Noyes. The article itself is well-written with interesting images of the subject. I would encourage you to visit it. The second insert is from book 00736 in my personal library and shows in pencil, the incredibly small handwriting of Marsha C. Noyes.
Sources:
1. "Marcia, Marcia, Marcia" MedChi Archives blog.
2. "Marcia C. Noyes, Medical Librarian" (PDF). Bulletin of the Medical Library Association. 35 (1): 108–109. 1947. PMC 194645
3. Smith, Bernie Todd (1974). "Marcia Crocker Noyes, Medical Librarian: The Shaping of a Career" (PDF). Bulletin of the Medical Library Association. 62 (3): 314–324. PMC 198800Freely accessible. PMID 4619344.
4. Edward Caledon BRUCE (1825-1901)"
5. Behind the scenes tour MedChiBuilding
"Clinical Anatomy Associates, Inc., and the contributors of "Medical Terminology Daily" wish to thank all individuals who donate their bodies and tissues for the advancement of education and research”.
Click here for more information
- Details
If you arrived to this website looking for information on Atrial Fibrillation, you will find some here and in this article.
Prevention of Stroke in Atrial Fibrillation;
Elimination of the Left Atrial Appendage.
An online educational video.
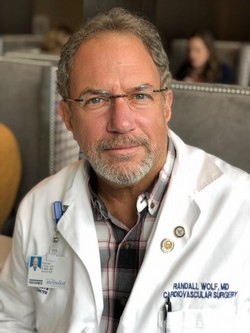
Randall, K. Wolf MD, FACS, FACC
This video educational program is hosted by the Houston Methodist DeBakey Heart and Vascular Center Education Center
Atrial fibrillation (AFib) is estimated to affect up to 4% of the population. Characterized by a rapid, irregular heartbeat, AFib is largely due to abnormal electrical impulses that cause the atria of the heart to quiver instead of beating steadily. Blood flow is reduced and is not completely pumped out of the two small upper chambers of the heart, the atria. This negatively impacts cardiac performance and also allows the blood to pool and potentially clot, especially in an extension of the left atrium, the left atrial appendage (LAA). At rest, a normal heart rate is approximately 60 – 100 beats per minute. In a person with AFib, that heart rate can increase to 180 bpm or even higher.
The main concern with AFib and stagnant blood flow in the LAA is the potential for clot formation (thrombus). While this can happen in either atria (right or left) the anatomy of the right atrium and right atrial appendage are less conducive to clot formation. The LAA is exactly the opposite and the clots, should they float into the bloodstream, tend to enter the larger arteries that go towards the head and brain, increasing the chances for a stroke.
In this educational video Dr. Wolf discusses the above, as well as the benefits of the elimination of the LAA, decreasing blood pressure, decreasing the chances of a stroke, and helping return the heart to normal rhythm.
Dr. Wolf is a surgical innovator who since the year 2000 has been a pioneer in the minimally invasive surgical treatment of AFib. He has performed over 2000 Wolf MiniMaze procedures since the first one in 2003 and has demonstrated the procedure to over 800 heart surgeons worldwide. He has been visiting professor in 18 countries, including Oxford University, University of Tokyo and Peking University. Dr. Wolf has delivered hundreds of invited lectures at hospitals, academic meetings and seminars in the United States and abroad.
Dr. Wolf is currently a member of the DeBakey Heart and Vascular Center at Houston Methodist Hospital in the Texas Medical Center. He serves as the arrhythmia specialist of the group. In 2018 Dr. Wolf operated on AF patients from 32 US states. He was also the keynote speaker at the annual Japanese Society for Tobacco Control in Takamatsu, Japan and the annual Chinese Society of Cardiothoracic Surgeons in Shenyang, China.
NOTE: Dr. Randall Wolf is a contributor to Clinical Anatomy Associates. My personal thanks to him and to the DeBakey Heart and Vascular Center for their invitation to participate in this and other educational videos. Dr. Miranda.
- Details
- Written by: Efrain A. Miranda, Ph.D.
This article is part of the series "A Moment in History" where we honor those who have contributed to the growth of medical knowledge in the areas of anatomy, medicine, surgery, and medical research.
William S. Halsted
mouseover for
Samuel J. Crowe
In my many years working with medical industry, surgeons, and surgery, I have heard many times that such and such surgical technique follows “Halsted’s Rules of Surgery”. The problem is that only two of these “rules” were mentioned and never did I receive an answer while working with Ethicon and Ethicon Endosurgery, and never did I receive an answer as to where could I find the reference regarding the other rules, if they even existed.
I recently read a great 1957 book by Samuel James Crowe, MD (1883-1952), titled “Halsted of John Hopkins; the man and his men”. Dr. Crowe lived for one year with Dr. William Stewart Halsted (1852-1922) and his wife as a medical student at John Hopkins. He was also an intern for Dr. Harvey Cushing, and although he wanted to follow Cushing into neurosurgery, Dr. Halsted placed him in charge of the newly created department of otolaryngology at John Hopkins, a position he did not want. Dr. Crowe went on to become a world-wide renown otolaryngologist.
Here are Halsted’s “Rules of Surgery” as explained by Dr. Crowe, based on Halsted’s research, experiments, and observations (with my own notes and comments):
1. Wounds are resistant to infection when no bits of tissue have been:
a. torn with clamps
b. torn by the rough handling of retractors
c. devitalized by hastily and carelessly applied ligatures
Note: this follows the ancient rule of “Primum Non Nocere”: first and foremost, do not harm
2. Wounds or parts rich in blood vessels usually heal without any visible granulation, even when no antiseptic precautions have been taken.
3. Incisions should be closed carefully and gently, layer by layer
4. The approximating sutures should never put the tissues under tension, since tension interferes with the blood supply and may cause necrosis
Note: Tension-avoidance surgical techniques follow this, one of the prime rules of surgery.
5. The end of the forceps used to pick up bleeding points should be small, to avoid crushing and destroying the vitality of surrounding tissues
Note: This observation led to the creation of fine, multiple toothed thumb forceps used today in cardiovascular surgery , such as the Cooley, DeBakey, Castaneda, etc. type forceps.
6. A drain is essential when there is necrotic tissue and infection
7. Silk should never be used in the presence of infection
Note: This makes sense. Since silk is an organic material, infected tissues will react to the presence of this extraneous material causing more inflammation, and the phagocytic cells in the tissues will destroy the silk and its capacity to hold the tissues together
8. The silk (suture) employed should never be coarser (larger gauge) than necessary and it is well to employ a suture a thread that is not stronger that the tissue it holds
9. A greater number of fine stitches is better than a few coarse ones
Note: This also makes sense. Halsted was known to be extremely meticulous and he could place a hundred stitches of fine silk thread where other surgeons would place a lesser number of coarser stitches. Using a larger number of fine stitches distributes the approximating tension of the sutures over a larger area, thus reducing the chance for suture dehiscence.
10. Avoid when possible the combined use of silk and catgut in a wound
11. For sewing up an abdominal wound, when it is necessary to take heavy deep stitches perforating skin and muscles, silver wire serves admirably
Note: Remember the times when these guiding principles where laid. Nylon, polypropylene, and other synthetic absorbable and non-absorbable sutures had yet to be discovered. Today the same dictum would probably say “For sewing up an abdominal wound, when it is necessary to take heavy deep stitches perforating skin and muscles, a synthetic non-absorbable suture material serves admirably”
It must be noted that Halsted never called the above the “rules of surgery”, rather they are observations that have become guiding principles. These have influenced the world of surgery to this day.
SIDE NOTE: It has been said many times that Dr. Halsted was the first to use rubber gloves. This is not true, Dr. Crowe says that “it was an evolution rather than a happy thought” and it involved his wife Caroline Hampton. This will be the subject of another article.
- Details
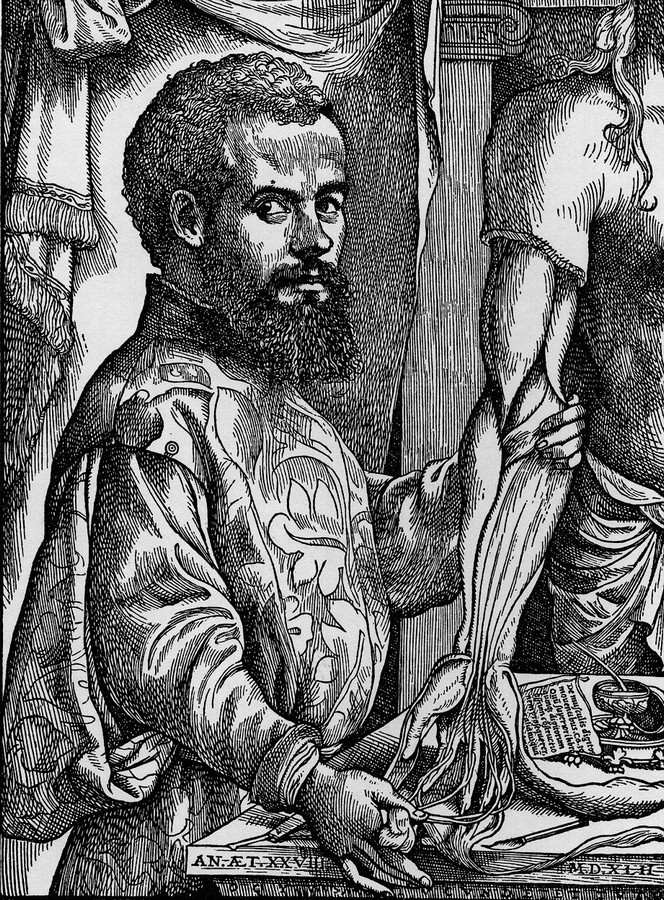
Figure 1: Vesalius Fabrica Portrait
Recently I acquired the 1925 book “The Iconography of Andreas Vesalius” by Marion Harry Spielmann (1858-1948). M.H. Spielmann was a well-published Victorian art scholar and critic. At the end of this article you can find the bibliographical information on this book.
The book is a serious detailed research of the known paintings, lithographies, sculptures, and medals that show the likeness of Andreas Vesalius, the date of publication and the author’s commentary on each one.
Andreas Vesalius is known as the “Father of Modern Anatomy”. He pushed for a description of the structure of the human body as seen in a dissection, going against the trend at the time where the anatomy was that described by Galen of Pergamon in his books. Galen’s anatomy was based on animal dissection and not a lot of human dissection. Furthermore, the lecturer would read from the book and the demonstrator pointing at the structures ignoring the discrepancies between the book and the body. For additional information and images click here.
Vesalius opus magnum (great work) was the publication in May 1543 of one of the most famous books in medical history. The title of the book is “De Humani Corporis Fabrica, Libri Septem” (Seven Books on the Structure of the Human Body). The book is now known as the “Fabrica”. This has led numerous artists to paint his likeness, many times based on past images or sometimes from pure imagination. The latest modern edition of the Fabrica was published in 2014.
We do know of only one portrait that depicts Vesalius’ likeness at the time of printing (1542) and that is the second image in the Fabrica of 1543 (figure 1) This image was carved in a pear wood block later used for printing. The woodblock indicates the date of carving (1542) and the age of the great anatomist that year (28). The sketch from which the block of wood was carved is most surely made by Jan Stephan Van Calcar (1449-1546). There is only supposition as to who was the artist that carved the woodblock, and there are several research papers on the subject. The best suggestion is that the woodcarvers were Francesco Marcolini (1505-1560) and Domenico Campagnola (1500-1564), both mentioned in a paper by Jaffe and Buchanan (2016). Campagnola is actually thought to be the woodcarver for the title page of the 1543 Fabrica.
The Iconography book goes into great detail on this image of the great anatomist, and dedicates a detailed description of the title page of the 1543 and the 1555 editions of the Fabrica, descriptions that I can only encourage to be read by researchers interested in the life and works of Andreas Vesalius. The book can be read online the Internet Archive here. The book is written mostly in English, but has an introduction in French.

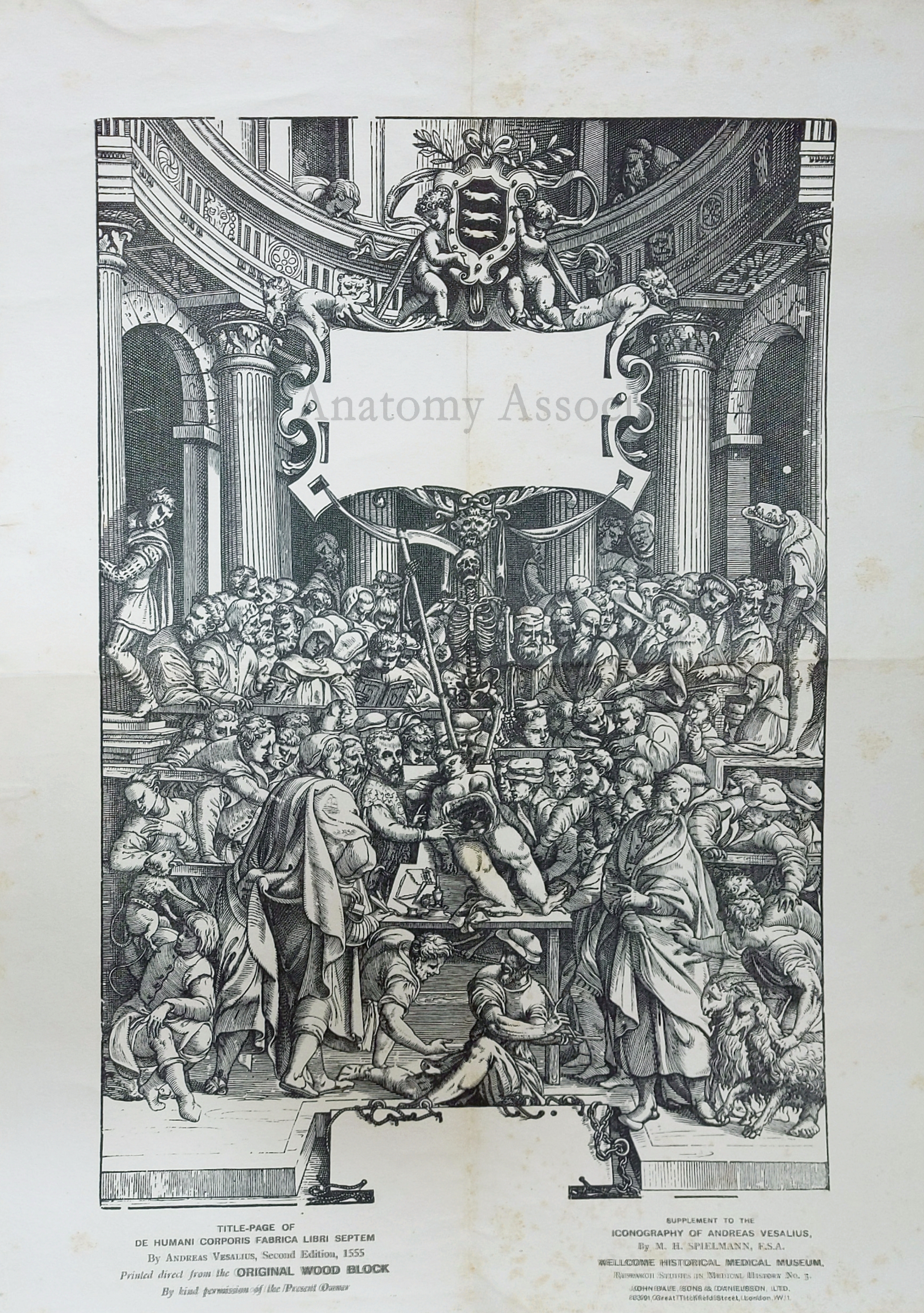
Figure 2: 1555 Fabrica Title Page
“The Iconography of Andreas Vesalius” is a rare book, it is not easy to find, and probably the most important characteristic of the book is not mentioned in the many descriptions of the book found on the Internet, medical libraries, and antiquarian booksellers websites: The book originally included a separate, folded-in-four, high-quality linen paper print of the title page of the 1555 Fabrica. Most of the books found today have lost this print. Figure 2 shows a scan of the print found in the book I acquired. A 4.5 Mb watermarked actual size of this print can be seen here. If you want to download it, you can right click on the image and then click on "Save As".
{kind=link}
This reprint of the Fabrica’s title page was done using the 1555 original woodblock, which makes it priceless. As shown in the accompanying image, the page leaves blank the two places where the title of the book and the dedication to the king and printer markings where placed. These would have been prepared in separate type and rearranged for a different use after printing. The print measures 16 7/8 by 12 1/4 inches (31.1 by 42.9 cms) The woodblock of the title page of the 1555 Fabrica was last used in 1934 when it was used to print the 1934 edition of the Icones Anatomicae, and then returned to the Louvain University in Belgium where it was destroyed by the German army in 1940. The Icones Anatomicae was the last print using the original woodblocks.
The rest of the original woodblocks was burned during a WWII bomb raid on July 16, 1944.
The following information is from the Stanford Library and it is one of the few that indicate the existence of the reprint of the 1555 Fabrica title page in an envelope pasted on the book cover reverse.
Author/Creator: Spielmann, M. H. (Marion Harry), 1858-1948.
Subject: Vesalius, Andreas, 1514-1564. History of Medicine. Physicians. 1500s
Genre: Biographical Information. Historical Works. Portraits
Bibliographic information:
Date: 1925
Series: Research studies in medical history ; no. 3, 1925
Note: Includes index. Title-page of De humani corporis fabrica libri septum by Andreas Vesalius, Second edition, 1555 printed direct from the original wood block in the pocket on verso of cover.
Personal Note: I am working on updating my library catalog to reflect the latest book acquisitions and gifts received. Dr. Miranda.
Sources:
1. “The Iconography of Andreas Vesalius” M.H. Spielmann. The Wellcome Historical Medical Museum London. John Bale, Sons & Danielson Ltd.
2. “The Andreas Vesalius Woodblocks: A Four Hundred Year Journey from Creation to Destruction” Acta Med Hist Adriat 2016; 14(2);347-372
3. "The identity of the artists involved in Vesalius Fabrica 1543” Guerra, F. (1969) Medical History, 13(1), 37.
- Details
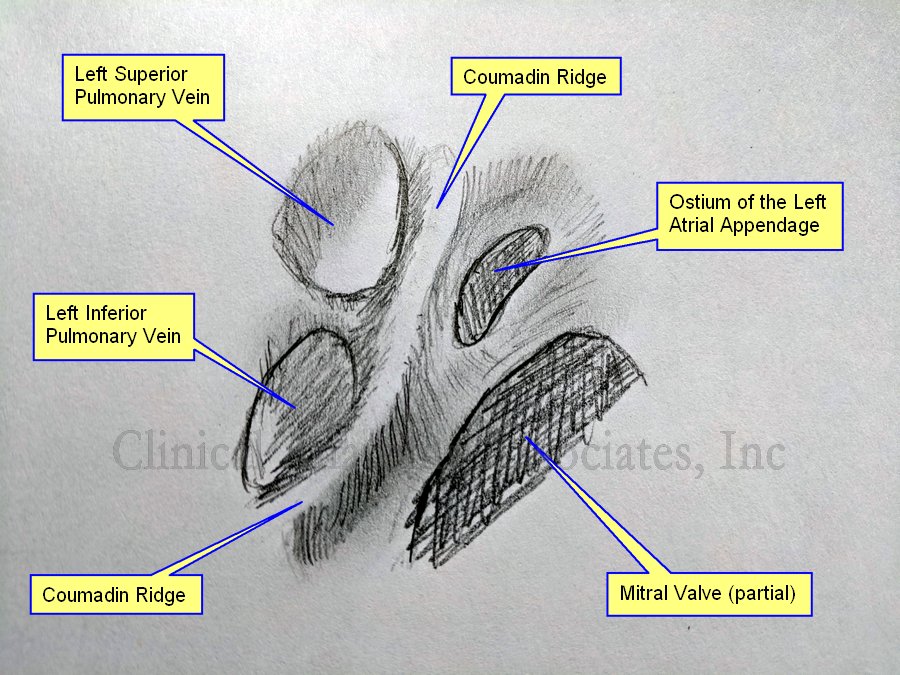
Coumadin ridge
Click on the image for a larger version
UPDATED: The [Coumadin ridge], also known as the [Warfarin ridge], or a [left atrial pseudotumor]. is an excessive elevation or protrusion of a normal ridge found between the left superior pulmonary vein and the internal ostium of the left atrial appendage. Usually this ridge will extend inferiorly towards and anterior to the ostium of the left inferior pulmonary vein. The Coumadin ridge is considered an anatomical variation of the otherwise small ridge, known as the left lateral ridge.
Because of its location and morphology, some cardiologists and radiologists have mistaken this elevation or fold of the internal anatomy of the left atrium for a thrombus and prescribed anticoagulant therapy (Coumadin or Warfarin) when none was needed, hence its name.
To understand the generation of the Coumadin ridge we must understand the embryology of this area of the heart. The left atrial appendage is the original left atrium in the embryo, which is displaced anteriorly and superolaterally when the veins that enter the atrium start to dilate at their distal end creating the left sinus venarum. After the left atrium proper has formed, the left atrial appendage is left as nothing more than an embryological remnant that can cause problems if the patient has atrial fibrillation (AFib). The ridge forms at the point where the left atrial appendage and the sinus venarum meet.
The Coumadin ridge can vary in morphology, from presenting as an elevated ridge, to a bulbous, pedunculated mass that seems to float within the left atrial appendage and undulate, following the cardiac motion, forcing the cardiologist into believing they are in the presence of a thrombus or a tumor within the heart.
This fold of tissue may contain the ligament of Marshall, autonomic nerves, and a small artery. In rare cases there may be an actual tumor arising from the location of the Coumadin ridge, but this is just a coincidence.
Now that the Coumadin ridge is a better known anatomical variation, cardiologist sometimes refer to their finding as a pseudotumor, a description that may scare the patient, but is only but a fold of tissue inside the heart.
Finding a Coumadin ridge in a patient with atrial fibrillation can be an interesting situation requiring differential diagnosis, as a patient with AFib can present with thrombi in the left atrial appendage. What to do? Is it or is it not a thrombus? Also, a differential diagnosis is needed in the case where the image is actually that of a left atrial tumor or an atrial myxoma.
The accompanying image is own work based on Sra (2004) and McKay (2008), and is a graphite on paper sketch. The image shown an internal view of the left atrium showing the left superior and inferior pulmonary vein, the ostium of the left atrial appendage and a segment of the area of the mitral valve.
We would like to thank Dr. Randall K Wolf, a contributor to Medical Terminology Daily for suggesting this article.
Sources:
1. “Coumadin ridge: An incidental finding of a left atrial pseudotumor on transthoracic echocardiography” Lohdi,AM, et al. World J Clin Cases. 2015 Sep 16; 3(9): 831–834
2. “Coumadin ridge” Tasco, V. https://radiopaedia.org/articles/coumadin-ridge
3. “Papillary fibroelastoma arising from the coumadin ridge” Malik, M, Shilo, K, Kilic,A. J Cardiovasc Thorac Res. 2017;9(2):118-120.
4. “‘Coumadin ridge’ in the left atrium demonstrated on three dimensional transthoracic echocardiography” McKay,T., Thomas, L. Europ J Echocard (2008) 9, 298–300
5. “Endocardial imaging of the left atrium in patients with atrial fibrillation” Sra J; Krum D; Okerlund D; Thompson H. J Cardiovasc Electrophysiol 2004 Feb; Vol. 15 (2), pp. 247
- Details
Continued from "The presence of Andreas Vesalius in Zakynthos (2)"
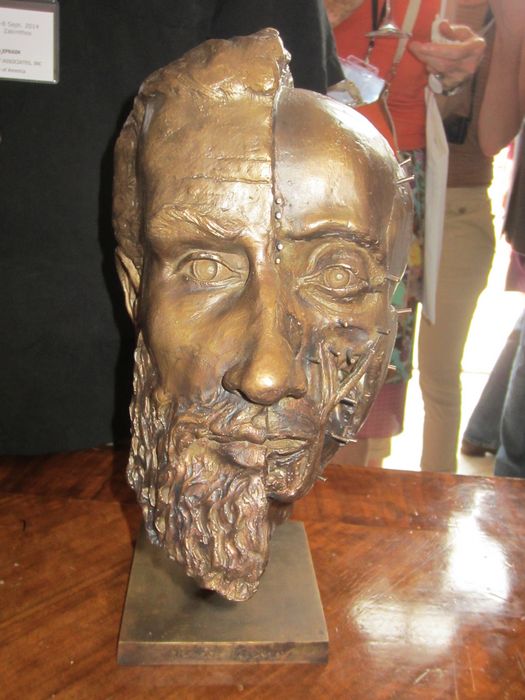
Bust of Vesalius made by Pascale Pollier
Bust of Vesalius made by Pascale Pollier
According to Theo Dirix, Belgian Consul to Greece and Vesalius enthusiast, there are other reminders on the island such as a painting in one of the local schools.
On September 3rd, 2014, as part of the Vesalius Continuum meeting on Zakynthos Island, a new bronze statue was unveiled to celebrate the life and works of Andrea Vesalius and remember his death on Zakynthos. This statue is a representation of Vesalius’ style of depicting anatomy in his book “De Humani Corporis Fabrica Libri Septem” and is a “muscle man” mixed with the motif of the famous plate 20 of Book 1 that shows a skeleton musing over a skull. The statue also presents the Vesalius family coat of arms. The statue is the work of Richard Neave and Pascalle Pollier.
Pascale Pollier, a biomedical artist specializes in face reconstructions and made a new bust of Vesalius based on the only known portrait of the great anatomist found on the pages of his immortal book “The Humani Corporis Fabrica Libri Septem”.
The statue was unveiled in front of an international crowd of anatomists, medical historians, biomedical artists, and film makers. Following the ceremony a display of artistic works related to Vesalius was opened in the Zakynthos municipality.
These are today the signs of the presence of Vesalius on Zakynthos. We know today that his body is interred in the cemetery of the church of Santa Maria della Grazie in Zakynthos. Sadly this church was destroyed twice in earthquakes and in 1953 was completely demolished along with 85% of the city. It was not rebuilt and now lies under the new, rebuilt city. One of the research papers presented at the 2014 Vesalius Continuum meeting has rediscovered the location of the church with great accuracy. The account of this paper and how I was able to find this geolocation will be presented in another article.
In 2014 the Vesalius Continuum Meeting with the Zakynthos government helped unveil a bronze statue to honor Andreas Vesalius. The statue reminds us of the "philosopher" of Jan Stephan Van Calcar, but in this case it is a muscle man contemplating a skull. At the base of the statue is the Vesalian coat of arms with the three weasels

New bronze statue of Vesalius

Close up of the new bronze statue of Vesalius
Sources
1. “Andreas Vesalius of Brussels 1514-1564” O’Malley, CD. Los Angeles 1965
2. "Andreas Vesalius; The Making, the Madman, and the Myth" Joffe, SN. Persona Publishing 2009
3. “In Search of Andreas Vesalius – The Quest for the Lost Grave” Dirix, T. Lanoo Campus Belgium 2014
- Details
Continued from “The presence of Andreas Vesalius in Zakynthos (1)”
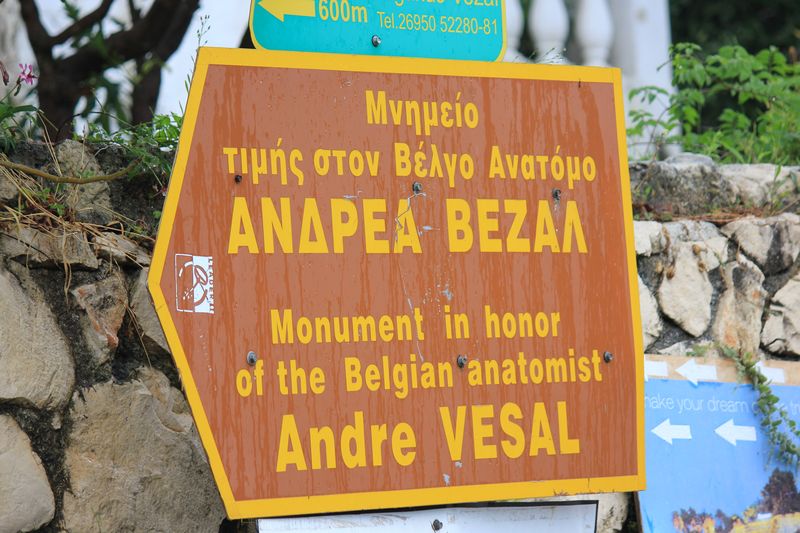
The second reminder of the presence of Andreas Vesalius in the Zakynthos Island is a street in the west side of the city of Laganas, “ΟΔΟΣ ΑΝΔΡΕΑ ΒΕΖΑΛ” or” Andrea Vesalius Street”. It is relatively short, narrow and windy, and it has several restaurants and hotels as you get closer to the sea where it ends at the beach. At this point there is a monument that honors Andrea Vesalius. This monument was erected in 1965. It has inscriptions in Greek, and Latin. This is the third memento to Vesalius in Zakynthos.

Vesalius street sign in Laganas
Directions to the Vesalius monument in Laganas

Vesalius Monument in Laganas
Vesalius Monument in Laganas
This monument was erected in Laganas following a legend that Vesalius had shipwrecked and he was found at the beach. Another legend says that Vesalius was left at the beach at Laganas to die as he was very sick. One of the presentations at the 2014 Vesalius Continuum meeting by Dr. Mauritz Biesbrouck disputed these legends with recently found letters by George Boucher to Johanes Metellus. George Boucher was a German jeweler that traveled with Vesalius back from Jerusalem and paid for Vesalius’ burial and monument at the church of Santa Maria della Grazie. These letters were authenticated and analyzed, bringing light to Vesalius’ place of disembarkment in Zakynthos. The Laganas monument, although correct in content, should be moved to the port of Zakynthos, to the point where the old city walls were found, the place where Vesalius collapsed and died.
The monument has a legend in both Greek and Latin. It reads as follows:
ΕΙΣ ΜΝΗΜΗΝ ΤΟΥ
ΑΝΔΡΕΑ ΒΕΖΑΛ
ΜΕΓΑΛΟΥ ΒΕΛΓΟΥ ΑΝΑΤΟΜΟΥ
ΘΑΝΟΝΤΟΣ ΕΝ ΖΑΚΥΝΘΩ ΤΟ 1564
Η ΕΝΩΣΙΣ ΤΩΝ ΔΙΠΛΜΑΤΟΥΧΩΝ ΤΩΝ
ΠΑΝΕΠΙΣΤΗΜΙΩΝ ΚΑΙ ΑΝΩΤΑΤΩΝ ΣΧΟΛΩΝ
ΤΟΥ ΒΕΛΓΙΟΥ, ΤΗΝ ΣΧΟΛΩΝ
ΑΝΗΓΕΙΡΕΝ ΤΘ 1965
IN MEMORIAM
ANDREAE VESALII BRUXELLENSIS
TUMULUS
QUI OBIIT IDIBUS OCTOBRIS ANNO MDLXIV
AETATIS VERO SUAE L
QUUM HIEROSOLYMIS REDISSET
Vesalii cineres venerandaque gentibus ossa
quisquis remota conteueris insula
qua jacer incultis memorosa Zakynthos arenis
gradum, viator et laborem sistito
naturae genium finemque extre maque rerum
vidisse credens coetera insanus labor
The rest is a poem in Latin that is translated as:
“The ashes and bones of Vesalius, sacred to the world
whoever finds then on this isolated island passing by the wild shores of Zakynthos,
should hold his tired steps, and believe that it is here that Vesalius met the ultimate goal of nature
and understood that striving for anything else is pointless” (Stouffis, Z, 1990)
When I visited this spot it was raining very hard and while I waited to take these pictures I looked out at the dark sea almost believing that maybe this was the spot where Vesalius came to land in Zakynthos. Now we know that it is not, but the moment was poignant and made me feel closer to the great anatomist.
On a more mundane note, in this area of Laganas because of the street name there are several businesses named "Vezal", a hotel, a supermarket and a taverna! I could not bring myself to post images of those places.
Continued in "The presence of Andreas Vesalius in Zakynthos (3)