![]()
Medical Terminology Daily (MTD) is a blog sponsored by Clinical Anatomy Associates, Inc. as a service to the medical community. We post anatomical, medical or surgical terms, their meaning and usage, as well as biographical notes on anatomists, surgeons, and researchers through the ages. Be warned that some of the images used depict human anatomical specimens.
You are welcome to submit questions and suggestions using our "Contact Us" form. The information on this blog follows the terms on our "Privacy and Security Statement" and cannot be construed as medical guidance or instructions for treatment.
We have 599 guests and no members online
")
Marcia Crocker Noyes
(1869 – 1946)
Further to my comment on old books and research that started with an interesting bookplate (Ex-Libris). I continued my research and found that the person in charge of the Osler library bookplate was a fascinating individual that today maybe a ghost in the MedChi library and building in Baltimore... This is certainly an article that can be called "A Moment in History"
Marcia Crocker Noyes was the librarian at The Maryland State Medical Society from 1896 to 1946 and was a founding member of the Medical Library Association.[1][2][3]
Sir William Osler, MD. a famous Johns Hopkins surgeon was a noted bibliophile and had a large personal collection of books on various topics. When he became the President of MedChi in 1896, he was dismayed at the condition of the library and knew that with the right person and some stewardship, it could become a significant collection. Sir William asked his friend, Dr. Bernard Steiner, a physician and President of the Enoch Pratt Free Library in Baltimore for suggestions of a librarian, and Dr. Steiner recommended Marcia Crocker Noyes. A native of New York, and a graduate of Hunter College, Marcia had moved to Baltimore for a lengthy visit with her sister, and took a “temporary” position at the Pratt Library, which turned into three years. Although she had no medical experience or background, she was enthusiastic, and most importantly, she was willing to move into the apartment provided for the librarian, who needed to be available 24 hours a day.
The image in this article is Ms. Noyes on her first year on the job. Marcia developed a book classification system for medical books, based on the Index Medicus, and called it the Classification for Medical Literature. The system uses the alphabet with capital letters for the major divisions of medicine and lower-case ones for the sub-sections. The system was used for many years, but it's now dated and the Faculty's original shelving scheme was never changed. The card catalogs still reflect her classification and many of the cards are written in Marcia's back-slanting handwriting.
Marcia knew enough to ask the Faculty's members about medical questions, terminology and literature. She gradually won over the predominantly male membership and they became her greatest allies; Sir William at the start, and then for nearly 40 years, Dr. John Ruhräh, a wealthy pediatrician with no immediate family of his own. She made a point of attending almost every Faculty function, and in 1904, under guidelines from the American Medical Association, Marcia was made the Faculty Secretary. For much of her first 10 years, she was the Faculty's only full-time employee, only being assisted by Mr. Caution, the Faculty's janitor. Later in life Marcia would say that she hired him because of his name!
Within ten years, the library had outgrown its space, and plans, spearheaded by Marcia and Sir William before his move to Oxford, were made to build a headquarters building, mainly to house the library's growing collection of medical books and journals.
Marcia was instrumental in the design and building of the new headquarters. She travelled to Philadelphia, New York and Boston to look at their medical society buildings, and eventually, the Philadelphia architectural firm, Ellicott & Emmart was selected to design and build the new Faculty building. Every detail of the building held her imprimatur, from the graceful staircase, to the light-filled reading room, and all of the myriad details of the millwork, marble tesserae, and most of all, the four-story cast iron stacks. She was on-site, climbing up unfinished staircases, checking out the progress of the building, which was built in less than one year at a cost of $90,000.
Among the features of the new building was a fourth-floor apartment for her. She referred to it as the "first penthouse in Baltimore" and it had a garden and rooftop terrace. The library collection eventually grew to more than 65,000 volumes from medical and specialty societies around the world. Journals were traded back and forth, and physicians eagerly anticipated the arrival of each new issue. At the same time, Marcia was involved in the Medical Library Association as one of eight founding members. The MLA promotes medical libraries and the exchange of information. One of the earliest mandates of the MLA was the Exchange, a distribution and trade service for those who had duplicates or little-used books in their collections. Initially, the Exchange was run out of the Philadelphia medical society, but in 1900 it was moved to Baltimore and Marcia oversaw it. Several hundred periodicals and journals were received and sent each month, a huge amount of work for a tiny staff. In 1904, the Faculty had run out of room to manage the Exchange, so it was moved to the Medical Society of the Kings County (Brooklyn). But without Marcia's excellent administrative skills, it floundered and in 1908, the MLA asked Marcia to take charge once again.
In 1909, when the new Faculty building opened, there was enough room to run the Exchange and with the help of MLA Treasurer, noted bibliophile and close friend, Dr. John Ruhräh, it once again became successful. Additionally, Marcia and Dr. Ruhräh combined forces to revive the MLA's bulletin, which had all but ceased publication in 1908, taking the Exchange with it. This duo maintained editorial control from 1911 until 1926. In 1934, around the time of Dr. Ruhräh's death, Marcia became the first “unmedicated” professional to head the MLA. During her tenure, the MLA incorporated, the first seal was adopted, and the annual meeting was held in Baltimore. Marcia wanted to write the history of the MLA once she retired from full-time work at the Faculty, but her health was beginning to fail. She had back problems and had suffered a serious burn on her shoulder as a young woman, possibly from her time running a summer camp, Camp Seyon, for young ladies in the Adirondack Mountains. In 1946, a celebration was planned to honor Marcia's 50 years at the Faculty. But she was adamant that the physicians wait until November, the actual date of her 50 years. However, they knew she was gravely ill, and might not make it until then, so a huge party was held in April. More than 250 physicians attended the celebration, but the ones she was closest to in the early years, were long gone. She was presented with a suitcase, a sum of money to use for travelling, and her favorite painting of Dr. John Philip Smith, a founder of the Medical College in Winchester, Virginia. It was painted by Edward Caledon Smith, a Virginia painter who had been a student of the painter Thomas Sully.[4] She adored this painting and vowed, jokingly, to take it with her wherever she went.
The painting was not to stay with her for very long, for she died in November 1946, and left it to the Faculty in her will. Her funeral was held in the Faculty's Osler Hall, named for her dear friend. More than 60 physicians served as her pallbearers, and she was buried at Baltimore's Green Mount Cemetery. In 1948, the MLA decided to establish an award in the name of Marcia Crocker Noyes. It was for outstanding achievement in medical library field and was to be awarded every two years, or when a truly worthy candidate was submitted. In 2014, the Faculty began giving a bouquet of flowers to the winner of the award in Marcia's name, and in honor of her work. Much evidence exists for this tradition, as we know that the physicians, especially Drs. Osler and Ruhräh, frequently gave her bouquets of flowers. Marcia also cultivated flower gardens at the Faculty and decorated the rooms with her work.
Today, the MedChi building is open for tours and if the rumors are to be believed Ms. Marcia Crocker Noyes is still at work in her beloved library as the "resident ghost" [1][5]

NOTE: This article has been modified from the original Wikipedia article on Marcia Crocker Noyes. The article itself is well-written with interesting images of the subject. I would encourage you to visit it. The second insert is from book 00736 in my personal library and shows in pencil, the incredibly small handwriting of Marsha C. Noyes.
Sources:
1. "Marcia, Marcia, Marcia" MedChi Archives blog.
2. "Marcia C. Noyes, Medical Librarian" (PDF). Bulletin of the Medical Library Association. 35 (1): 108–109. 1947. PMC 194645
3. Smith, Bernie Todd (1974). "Marcia Crocker Noyes, Medical Librarian: The Shaping of a Career" (PDF). Bulletin of the Medical Library Association. 62 (3): 314–324. PMC 198800Freely accessible. PMID 4619344.
4. Edward Caledon BRUCE (1825-1901)"
5. Behind the scenes tour MedChiBuilding
"Clinical Anatomy Associates, Inc., and the contributors of "Medical Terminology Daily" wish to thank all individuals who donate their bodies and tissues for the advancement of education and research”.
Click here for more information
- Details

Click for a larger image
The word acetabulum is formed by the combination of the Latin root [acetum], meaning "vinegar", and the Latin suffix [-abulum] a diminutive of [abrum], meaning a "cup", "holder", or "receptacle". Thus formed, the word acetabulum means "a small vinegar cup".
Roman soldiers liked to drink their water mixed with a small quantity of vinegar, so as to reduce the sensation of thirst. This mix was called "Posca". An acetabulum was used to add specific quantities of vinegar to the water, so over time the acetabula (plural form of acetabulum) were considered measuring devices. It is said that they measured one cup, or 2 1/2 oz. of wine.
The anatomical acetabula are bilateral cup-like depressions in the os coxae which serve as a component of the coxofemoral joint (hip joint). They are found at the intersection of the three bony components of the os coxae, the ilium, ischium, and pubic bone and look anteroinferiorly.
The acetabulum has several components:
• Acetabular margin: An incomplete circular bony edge or border that marks the edge of the acetabulum
• Acetabular notch: The area where the acetabular margin is incomplete
• Acetabular labrum: Labrum (Lat. :lip). The acetabular labrum is a complete circular ring of fibrocartilage found on the acetabular margin that helps maintain the head of the femur in place. It is not shown in the accompanying image
• Lunate surface: A smooth, half-moon shaped area on the floor of the acetabulum. It is covered with hyaline cartilage and allows for articulation with the head of the femur
• Acetabular fossa: The non-articular region of the floor of the acetabulum. It contains fat, vessels, and the ligament of the head of the femur
Interesting fact: You may find that in older English anatomy books the acetabulum is referred to as the cotyloid cavity. The word cotyloid arises from the Greek [κοτυλοειδές] and means "similar to a cup". This separation in terms still exists when studying anatomy in other languages. For example, in Spanish the acetabulum is called "cavidad cotiloídea" or "cotilo", and in French it is called "cavité cotyloïde" or "cotyle". I guess the Greek soldiers did not drink vinegar with their water...
Image property of: CAA, Inc. Photographer: David M. Klein
- Details
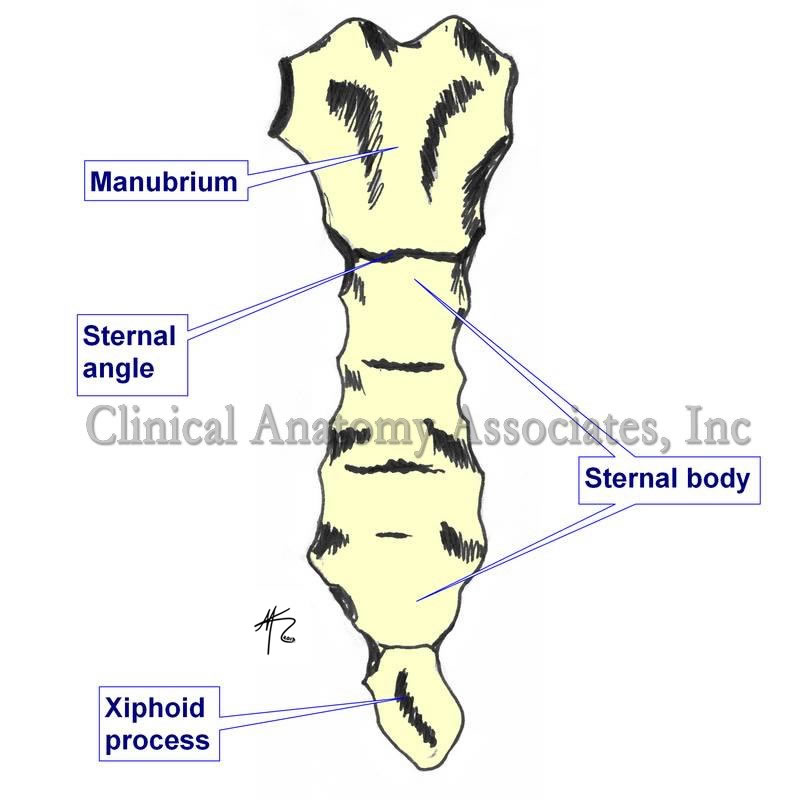
Sternum, anterior view
UPDATED:The sternal angle is the term used to denote the angulation at the joint between the manubrium and the body of the sternum. This transverse joint is called the "manubriosternal joint" and is a secondary cartilaginous joint of a type known as a symphysis. The angle varies between 160 and 169 degrees.
It is know eponymously as the "angle of Louis" named after Antoine Louis1 (1723-1792), a French physician. The importance of the sternal angle is that of an anatomical superficial landmark, which forms a horizontal plane which indicates a series of anatomical occurrences, as follows:
• Location of the cartilages of the second rib
• Beginning and end of the aortic arch
• Boundary between the inferior and superior mediastinum
• Location of the bifurcation of the trachea
• Posteriorly, the plane of the sternal angle passes trough the T4-T5 intervertebral disc (sometimes a little lower, through the superior aspect of T5)
• Highest point of the pericardial sac.
• It is the point where the right and left pleurae meet in the midline. They touch, but their pleural spaces do not communicate (usually).
1. Some authors contest the eponym, adjudicating it to Pierre Charles Alexander Louis (1787-1872), another French physician.
Image property of: CAA.Inc.. Artist: David M. Klein
Thoracic anatomy, pathology and surgery, are some of the many lecture topics developed and presented by Clinical Anatomy Associates, Inc. For more information Contact Us.
- Details
- Written by: Pascale Pollier
Cover of the book by Theo Dirix
My partner in crime and fellow traveler, Theo Dirix, has just published a new account of our common quest for the lost grave of Andreas Vesalius. Until the scientific results of our latest mission in Zakynthos in September 2017, will become public, this collection of articles published since 2014 represents a detailed and complete status quaestionis of a search that will never be the same anymore.
I'm proud and grateful to be part of a team he describes a most tenacious.
Following is a remarkable quote from the book: "The beast you have in your hands may appear as aged and stubborn: indeed, the texts collected here are not new and they regularly echo each other. The beast barks and growls: these words do not intend to examine or research but were meant to sell a project to potential sponsors. I feel the taste of the creature’s spit in my face, but pleading not guilty to any accusation of self-glorification, I do hope I managed to teach it a few tricks you will enjoy. While continuing to write about Vesalius’s death and his grave, black dogs may still be scratching at my hermitage. When I will finally throw open the doors to the beauty beyond, here’s hoping the encounter with the female spider will taste as fresh as a first kiss and be the beginning of something else."
No surprise some have described the book as: "a truly captivating story (a Live Adventure!) written in a fascinating, passionate and inspiring way. Theo Dirix, with his unique style is describing facts from his adventure to locate the grave of Vesalius and he is mentioning with great respect all his collaborators, the friends of Vesalius and those who share the same passion for Anatomy and Art." (Vasia Hatzi on Med in Art).
The book can be ordered here: https://www.shopmybooks.com/US/en/book/theo-dirix-32/in-search-of-andreas-vesalius. (English version of the website). More information about the author on his website www.theodirix.com. or here.
Personal note: Thanks to Pascale Pollier, a contributor to this website, for allowing us to publish this article, originally published on Vesalius Continuum.
I received a personalized copy from the author, Theo Dirix; Thank you very much for the recognition and the use of this website as reference in some of your comments. It is a great read for anyone even mildly interested in the life and specially the death and disappearance of the grave of Andreas Vesalius. There are several passages in the book that I will have to research and transform in articles for this blog.
For those who collaborated in the GoFundMe campaign because or our article entitled Do you want your name in a book? The Quest for the Lost Grave.... this is the book and the name of all the contributors are listed in it!
The quest continues... Dr. Miranda
- Details
- Written by: Randall K. Wolf, MD.
If you arrived to this article looking for information on Atrial Fibrillation, you will find some in this article. If you need to contact Dr. Wolf, please click here.
 Dr. Randall K. Wolf
Dr. Randall K. Wolf
HOUSTON AFib PATIENT EXPERIENCE SEMINAR
Saturday, April 21st, 2018 9am – 4pm
Westin at Memorial City, 945 Gesner Rd.
Houston, TX 77024
877-900-AFIB (2342)
This seminar is free and open to the public. To attend, please call the telephone number to register.
WELCOME MESSAGE FROM DR. RANDALL WOLF
In my experience over the last 18 years as a physician who specializes in the treatment of Atrial fibrillation (AFib), I have learned AFib sufferers want two things: Hope and a chance to feel better.
The first step to hope and to feeling better is to self educate. Learn about the latest medications, techniques and devices to treat AFib. Ask questions. Get a second opinion. Take charge of your health.
The purpose of the Houston AFib Patient Experience Seminar is to help AFib sufferers like you take charge of your health.
About 30 million people worldwide carry an AFib diagnosis. Today seems everyone either has AFib or knows someone that has AFib. When I first held an Afib seminar in Beijing, China, over 1200 people with AFib signed up for the seminar. It was standing room only!
Despite the common occurrence of AFib around the world, a recent study found that in patients who were diagnosed with AFib, 40-50% of patients with an elevated risk of stroke were not treated with the best therapy, and the rate of stroke over the next five years was 10%.
Here in Houston, we can do better! Learn more about AFib right here today, and I guarantee you will have hope and be more likely to reach your goal of feeling better.
Towards an AFib free healthy life,
Randall K. Wolf, MD.
ABOUT THE HOUSTON AFIB PATIENT EXPERIENCE SEMINAR
The University of Texas McGovern Medical School, Cardiothoracic and Vascular Surgery Department in Houston, is proud to host the inaugural Houston AFIB Patient Experience Seminar. The purpose is to educate the public in an interactive format allowing the audience to engage in conversation in a question/answer format with leading medical professionals. Our list of panel members and guest presentations include surgeons, cardiologists, neurologists, pulmonologists as well as testimonials from AFib patients. We are honored to be able to bring awareness to the resources and options available to patients suffering from AFIB.
NOTE: If you cannot attend the seminar, there is more information on Atrial Fibrillation at this website; click here.
- Details
This article is part of the series "A Moment in History" where we honor those who have contributed to the growth of medical knowledge in the areas of anatomy, medicine, surgery, and medical research.
This article continues the musings of "Interesting discoveries in a medical book". In this book I found a copy of a letter written by Ephraim McDowell, MD; who on December 25, 1809 performed the first recorded ovariotomy in the world. The patient was Mrs. Jane Todd Crawford, who has also been the subject of several articles in this website, including a homage to the "unknown patient/donor".
The book belonged to Cecil Striker, MD, who practiced in Cincinnati. Dr. Striker was a faculty at the University of Cincinnati and one of the founders of the American Diabetes Association (ADA). He also was one of the first physicians to work in 1923 with a "newly discovered" drug by the Eli Lilly Company (Indianapolis) this drug was named Insulin. The medical application of Insulin had only just been discovered about a year earlier.
 Inside the book there is a copy of a letter by Dr. Ephraim McDowell to Dr. Robert Thompson dated January 2nd, 1829, a year before Dr. McDowell's death. At the time (1829) Dr. Thompson (Sr.) was a medical student in Philadelphia. According to the note Dr. Thompson lived in Woodford County, KY, had three children and died in 1887. One of his children was also a doctor, but I have not been able to ascertain if this book was given to him by Dr. Striker.
Inside the book there is a copy of a letter by Dr. Ephraim McDowell to Dr. Robert Thompson dated January 2nd, 1829, a year before Dr. McDowell's death. At the time (1829) Dr. Thompson (Sr.) was a medical student in Philadelphia. According to the note Dr. Thompson lived in Woodford County, KY, had three children and died in 1887. One of his children was also a doctor, but I have not been able to ascertain if this book was given to him by Dr. Striker.
The letter is shown in the image attached. In this letter Dr. McDowell describes in his own words the ovariotomy he performed on Jane Todd. He also describes other ovariotomies he performed and his opinion on "peritoneal inflammation".
Note how the letter has no paragraph separation. Apparently, at the time writing paper was expensive and the less pages used, the better! The text of the letter is as follows:
Danville, January 2, 1829
Mr. Robert Thompson
Student of Medicine
No. 59 Spruce Street
Philadelphia, Pennsylvania
Sir,
At the request of your father I take the liberty of addressing you a letter giving you a short account of the circumstances which lead to the first operation for diseased ovaria. I was sent in 1809 to deliver a Mrs. Crawford near Greentown of twins; as the two attending physicians supposed. Upon examination per vaginam I soon ascertained that she was not pregnant; but had a large tumor in the abdomen which moved easily from side to side. I told the lady that I could do her no good and carefully stated to her, her deplorable situation. Informed her that John Bell, Hunter, Hay, and A. Wood four of the first and most eminent surgeons in England and Scotland had uniformly declared in their lectures that such was the danger of peritoneal inflammation, that opening the abdomen to extract the tumor was inevitable death. But not standing with this, if she thought herself prepared to die, I would take the lump from her if she would come to Danville. She came in a few days after my return home and in six days I opened her side and extracted one of the ovaria which from its diseased and enlarged state weighed upwards of twenty pounds. The intestines as soon as an opening was made run out upon the table, remained out about twenty minutes and being upon Christmas Day they became so cold that I thought proper to bathe them in tepid water previous to my replacing them; I then returned them, stitched up the wound and she was perfectly well in 25 days. Since that time I have operated eleven times and have lost but one. I now can tell at once when relief can be obtained by an examination of the tumor if it floats freely from side to side or appears free from attachments except of the lower part of the abdomen. I advise the operation, having no fear from the inflammation that may ensue. I last spring operated upon a Mrs. Bryant from the mouth of the Elkhorn from below Frankfort. I opened the abdomen from the umbilicus to the pubis and extracted sixteen pounds. The said contained the most offensive water I ever smelt, and the attendants puked or discharged except myself. She is now living; from being successful in the above operation. Several young gentlemen with ruptures have come to me. I have uniformly cut the ring open, put the intestines up if down the cut the ring all around, every quarter of an inch then pushed the parts closely together and in every case the cure has been perfect. Therefore it appears to me a mere humbug about the danger of the peritoneal inflammation. Much talked about by most surgeons. After wishing you Health and Happiness,
I am yours sincerely
E. McDowell
P.S. Your father looks better than I have ever seen. Your sister is also in health
The most important point of this letter is how easily and publicly they name patients and their home addresses. Today this would be a violation of the Health Insurance Portability and Accountability Act of 1996, commonly known as HIPPA, a legislation that provides data privacy and security provisions to safeguard patient medical information.
It is also interesting to see how Dr. McDowell explained to Mrs. Crawford how difficult and dangerous the procedure would be. He stated how four renown surgeons in England and Scotland said that opening the abdomen was "inevitable death". Another point was how long the intestines were outside the body ... twenty minutes, and the maneuver Dr. McDowell used to bring them back to normal temperature. Late December in Kentucky is quite cold, even with wooden stoves and such. I wonder how much the lower temperature helped the patient.
The last point refers to his success in hernia procedures in young males. In the 1800's the word "rupture" was the standard to name abdominal hernias. Without explaining the procedure in detail, Dr. McDowell says that "every cure has been perfect". At the time, this was unprecedented, as the recurrence of inguinal hernia procedures, when attempted, was close to 25%.
The house where Dr. McDowell lived and practiced is today a museum in Danville, KY. In February, 2017 I visited this museum and wrote an extensive article on it. I encourage those interested in the History of Medicine to visit the place.
- Details

Change the text of the image
UPDATED: [Pes anserinus] is the name given to a tri-flanged structure formed by the attachment of the flattened tendons of three muscles to the anteromedial surface of the superior aspect of the shaft of the tibia. The tendons correspond to the sartorius, the gracilis, and the semitendinosus muscles. The pes anserinus is related superficially to the the tibial insertion of the medial collateral ligament of the knee.
There is a bursa deep to these tendons, the [bursa anserinus], which can be the cause of painful bursitis.
The term [pes anserinus] literally means “goose foot”, as early anatomists compared this structure to the foot of this bird. In Latin [pes] means “foot”, and [anserinus] or [anser] means “goose”.
For other anatomical structures whose names are related to birds, click here.
Thanks to Jackie Miranda-Klein for suggesting this post. Jackie is studying for the Physician Assistant Master's degree at Kettering College. Dr. Miranda.
Image modified from the original: "3D Human Anatomy: Regional Edition DVD-ROM." Courtesy of Primal Pictures