![]()
Medical Terminology Daily (MTD) is a blog sponsored by Clinical Anatomy Associates, Inc. as a service to the medical community. We post anatomical, medical or surgical terms, their meaning and usage, as well as biographical notes on anatomists, surgeons, and researchers through the ages. Be warned that some of the images used depict human anatomical specimens.
You are welcome to submit questions and suggestions using our "Contact Us" form. The information on this blog follows the terms on our "Privacy and Security Statement" and cannot be construed as medical guidance or instructions for treatment.
We have 461 guests and no members online
")
Marcia Crocker Noyes
(1869 – 1946)
Further to my comment on old books and research that started with an interesting bookplate (Ex-Libris). I continued my research and found that the person in charge of the Osler library bookplate was a fascinating individual that today maybe a ghost in the MedChi library and building in Baltimore... This is certainly an article that can be called "A Moment in History"
Marcia Crocker Noyes was the librarian at The Maryland State Medical Society from 1896 to 1946 and was a founding member of the Medical Library Association.[1][2][3]
Sir William Osler, MD. a famous Johns Hopkins surgeon was a noted bibliophile and had a large personal collection of books on various topics. When he became the President of MedChi in 1896, he was dismayed at the condition of the library and knew that with the right person and some stewardship, it could become a significant collection. Sir William asked his friend, Dr. Bernard Steiner, a physician and President of the Enoch Pratt Free Library in Baltimore for suggestions of a librarian, and Dr. Steiner recommended Marcia Crocker Noyes. A native of New York, and a graduate of Hunter College, Marcia had moved to Baltimore for a lengthy visit with her sister, and took a “temporary” position at the Pratt Library, which turned into three years. Although she had no medical experience or background, she was enthusiastic, and most importantly, she was willing to move into the apartment provided for the librarian, who needed to be available 24 hours a day.
The image in this article is Ms. Noyes on her first year on the job. Marcia developed a book classification system for medical books, based on the Index Medicus, and called it the Classification for Medical Literature. The system uses the alphabet with capital letters for the major divisions of medicine and lower-case ones for the sub-sections. The system was used for many years, but it's now dated and the Faculty's original shelving scheme was never changed. The card catalogs still reflect her classification and many of the cards are written in Marcia's back-slanting handwriting.
Marcia knew enough to ask the Faculty's members about medical questions, terminology and literature. She gradually won over the predominantly male membership and they became her greatest allies; Sir William at the start, and then for nearly 40 years, Dr. John Ruhräh, a wealthy pediatrician with no immediate family of his own. She made a point of attending almost every Faculty function, and in 1904, under guidelines from the American Medical Association, Marcia was made the Faculty Secretary. For much of her first 10 years, she was the Faculty's only full-time employee, only being assisted by Mr. Caution, the Faculty's janitor. Later in life Marcia would say that she hired him because of his name!
Within ten years, the library had outgrown its space, and plans, spearheaded by Marcia and Sir William before his move to Oxford, were made to build a headquarters building, mainly to house the library's growing collection of medical books and journals.
Marcia was instrumental in the design and building of the new headquarters. She travelled to Philadelphia, New York and Boston to look at their medical society buildings, and eventually, the Philadelphia architectural firm, Ellicott & Emmart was selected to design and build the new Faculty building. Every detail of the building held her imprimatur, from the graceful staircase, to the light-filled reading room, and all of the myriad details of the millwork, marble tesserae, and most of all, the four-story cast iron stacks. She was on-site, climbing up unfinished staircases, checking out the progress of the building, which was built in less than one year at a cost of $90,000.
Among the features of the new building was a fourth-floor apartment for her. She referred to it as the "first penthouse in Baltimore" and it had a garden and rooftop terrace. The library collection eventually grew to more than 65,000 volumes from medical and specialty societies around the world. Journals were traded back and forth, and physicians eagerly anticipated the arrival of each new issue. At the same time, Marcia was involved in the Medical Library Association as one of eight founding members. The MLA promotes medical libraries and the exchange of information. One of the earliest mandates of the MLA was the Exchange, a distribution and trade service for those who had duplicates or little-used books in their collections. Initially, the Exchange was run out of the Philadelphia medical society, but in 1900 it was moved to Baltimore and Marcia oversaw it. Several hundred periodicals and journals were received and sent each month, a huge amount of work for a tiny staff. In 1904, the Faculty had run out of room to manage the Exchange, so it was moved to the Medical Society of the Kings County (Brooklyn). But without Marcia's excellent administrative skills, it floundered and in 1908, the MLA asked Marcia to take charge once again.
In 1909, when the new Faculty building opened, there was enough room to run the Exchange and with the help of MLA Treasurer, noted bibliophile and close friend, Dr. John Ruhräh, it once again became successful. Additionally, Marcia and Dr. Ruhräh combined forces to revive the MLA's bulletin, which had all but ceased publication in 1908, taking the Exchange with it. This duo maintained editorial control from 1911 until 1926. In 1934, around the time of Dr. Ruhräh's death, Marcia became the first “unmedicated” professional to head the MLA. During her tenure, the MLA incorporated, the first seal was adopted, and the annual meeting was held in Baltimore. Marcia wanted to write the history of the MLA once she retired from full-time work at the Faculty, but her health was beginning to fail. She had back problems and had suffered a serious burn on her shoulder as a young woman, possibly from her time running a summer camp, Camp Seyon, for young ladies in the Adirondack Mountains. In 1946, a celebration was planned to honor Marcia's 50 years at the Faculty. But she was adamant that the physicians wait until November, the actual date of her 50 years. However, they knew she was gravely ill, and might not make it until then, so a huge party was held in April. More than 250 physicians attended the celebration, but the ones she was closest to in the early years, were long gone. She was presented with a suitcase, a sum of money to use for travelling, and her favorite painting of Dr. John Philip Smith, a founder of the Medical College in Winchester, Virginia. It was painted by Edward Caledon Smith, a Virginia painter who had been a student of the painter Thomas Sully.[4] She adored this painting and vowed, jokingly, to take it with her wherever she went.
The painting was not to stay with her for very long, for she died in November 1946, and left it to the Faculty in her will. Her funeral was held in the Faculty's Osler Hall, named for her dear friend. More than 60 physicians served as her pallbearers, and she was buried at Baltimore's Green Mount Cemetery. In 1948, the MLA decided to establish an award in the name of Marcia Crocker Noyes. It was for outstanding achievement in medical library field and was to be awarded every two years, or when a truly worthy candidate was submitted. In 2014, the Faculty began giving a bouquet of flowers to the winner of the award in Marcia's name, and in honor of her work. Much evidence exists for this tradition, as we know that the physicians, especially Drs. Osler and Ruhräh, frequently gave her bouquets of flowers. Marcia also cultivated flower gardens at the Faculty and decorated the rooms with her work.
Today, the MedChi building is open for tours and if the rumors are to be believed Ms. Marcia Crocker Noyes is still at work in her beloved library as the "resident ghost" [1][5]

NOTE: This article has been modified from the original Wikipedia article on Marcia Crocker Noyes. The article itself is well-written with interesting images of the subject. I would encourage you to visit it. The second insert is from book 00736 in my personal library and shows in pencil, the incredibly small handwriting of Marsha C. Noyes.
Sources:
1. "Marcia, Marcia, Marcia" MedChi Archives blog.
2. "Marcia C. Noyes, Medical Librarian" (PDF). Bulletin of the Medical Library Association. 35 (1): 108–109. 1947. PMC 194645
3. Smith, Bernie Todd (1974). "Marcia Crocker Noyes, Medical Librarian: The Shaping of a Career" (PDF). Bulletin of the Medical Library Association. 62 (3): 314–324. PMC 198800Freely accessible. PMID 4619344.
4. Edward Caledon BRUCE (1825-1901)"
5. Behind the scenes tour MedChiBuilding
"Clinical Anatomy Associates, Inc., and the contributors of "Medical Terminology Daily" wish to thank all individuals who donate their bodies and tissues for the advancement of education and research”.
Click here for more information
- Details
![Torus - By LucasVB [Public domain], via Wikimedia Commons](/images/MTD/LargeImages/torus_lg.jpg)
Click for a larger image
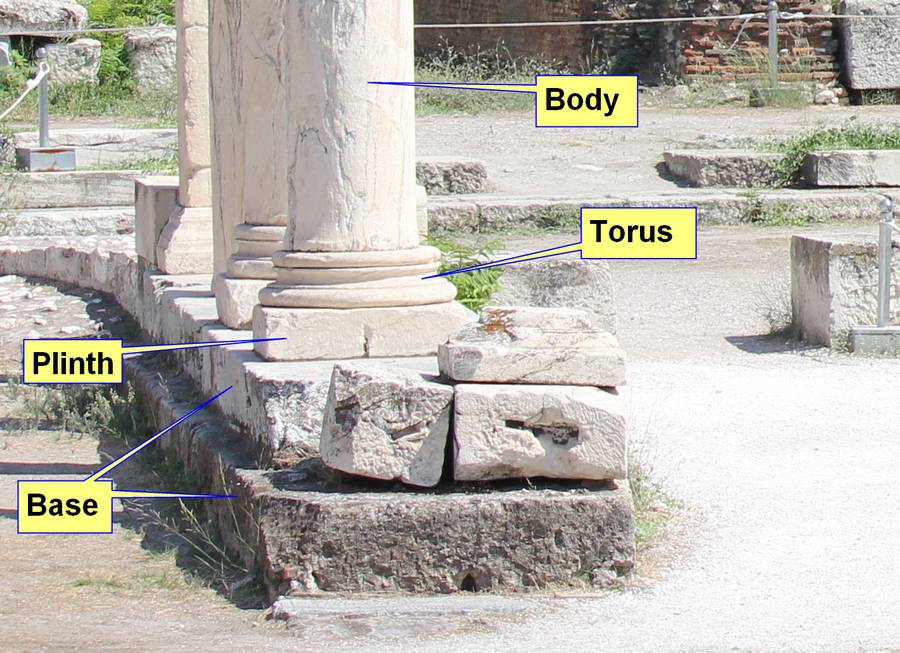
The word [torus] is of Latin origin and refers to “a rounded protuberance or swelling”. In science, it refers to a doughnut-shaped structure (see image). It also refers to the rounded, bulging, and circular base component of a pillar, found between the square plinth and the main body of the pillar. The torus can be seen in Egyptian, Greek, and Roman style pillars.
The term is used in anatomy and medicine to denote normal or abnormal circular or semicircular protuberances, as in the case of the “torus tubarius”, a normal semicircular elevation found at the ostium of the auditory tube (of Eustachius) in the lateral walls of the rhinopharynx. The torus tubarius elevation is due to the presence of lymphoid tissue which can get inflamed.
Torus mandibularis. An exostosis that develops on the inner side of the mandible
Torus palatinus: a benign, small exostosis that appears in the midline of the hard palate
In orthopedics it is used to denote a compression fracture where the cortex of a long bone close to one of its epiphyses buckles under longitudinal (axial) compression. The look of the fracture is similar to the location of the torus in a pillar. An example of this is the torus fracture (also known as buckle fractures) in children.
The term [torulus] is related to [torus], as it means a “small torus” and it refers to a small elevation, which is synonymous with the word “papilla”. An example of this is the term torulus tactiles palmaris, referring to small elevations on the palms of the hand. Another related term is [torulosis], referring to a large number of small elevations or pimples.
The following images are of a Greek pillar taken in 2014 in Athens showing the location of the torus. The next image shows a torus fracture. The image is from www.kidsfractures.com/forearm/ and we thank them for sharing the image with us. This is a great site for information on fractures in children.
Click for a larger view

Click for a larger view
Sources:
1. “Medical Meanings: A Glossary of Word Origins” Haubrich, WS. Am Coll Phys. Philadelphia 1997
2. “The Origin of Medical Terms” Skinner, HA 1970, New York. Hafner Publishing Company
3. “Taber’s Cyclopedic Medical Dictionary” 16th Ed. 1989. Philadelphia. FA Davis Company
4. www.kidsfractures.com/forearm/
Torus image: By LucasVB [Public domain], via Wikimedia Commons
Thanks to Jackie Miranda-Klein for suggesting this post. Dr. Miranda.
- Details

Excised bicuspid aortic leaflets
The normal components of the aortic valve are part of the aortic root. The valve is composed of three leaflets, each of which are related to a sinus of Valsalva, and three interleaflet triangles. The anatomy of the aortic root, the aortic valve and the interleaflet triangles of the aortic root have been described in other articles in this website.
A bicuspid aortic valve (BAV) is probably the most common cardiac defect of congenital origin. The prevalence of BAV ranges from 0.9% to 2% in the general population with a 3:1 male-female ratio.
In spite of the anomaly, a BAV may achieve normal valvular function, but this probably does not last, as BAV tend to develop calcifications in the adult leading to valvular disease, dysfunction, valvar stenosis, so complications are common, the most common being dilation of the aortic root and ascending aorta.
The etiology of a BAV is commonly accepted as congenital and there are some studies that demonstrate a familial component, but it can appear in families where there is no known history of BAV.
There are several attempts at classifying BAV, as the leaflets that fuse are different, and so is the way of fusion.
There is one rare BAV called “pure”. This purely BAV is a true BAV, composed of two leaflets of similar size where there is no clear fusion line or “raphe” between the fused leaflets (see image). This valve has two well developed interleaflet triangles and the third can be absent or vestigial. The image depicts the excised calcified leaflets where the left and right coronary cusps are fused.
Other types of BAV have a well-developed raphe, have two well developed interleaflet triangles and the third may be large or anomalous. The leaflets may also be asymmetrical. The classification of the different types of BAV goes beyond the objective of this article, but they can be studied in the references at the end of this article. There is no doubt that the different types of BAV can cause valvar disease and hemodynamic chaos, so the surgical approach for these may be different, including valve repair, aortic annuloplasty, interleaflet triangle remodeling, and of course valve removal and prosthetic implant, either biological or mechanical.
Clinically, the pathologies related to the function of the aortic valve are stenosis, valvular incompetence, and in some cases intimal aortic dissection, which is a catastrophic complication. Some of these complications are triggered by the calcification of the bicuspid leaflets. Interestingly, although BAV is a congenital disease, only one in fifty children known to have BAV have clinically significant disease by adolescence.
PERSONAL NOTE: I have permission to publish the image in this article… because the bicuspid aortic valve depicted in this article is my own. My personal thanks to the medical and support personnel at the Memorial Hermann Heart & Vascular Institute, in Houston, TX., and my three cardiovascular physicians without whom I would not be back writing this article, Drs. Randall K. Wolf (contributor to this website), Dr. William Ross Brown (cardiologist), and Dr. Tuyen (Tom) Nguyen, who operated on me. Dr. Miranda.
Sources:
1. “Etiology of bicuspid aortic valve disease: Focus on hemodynamics: Atkins, SA, Sucosky, P World J Cardiol. 2014 Dec 26; 6(12): 1227–1233.
2. “A classification system for the bicuspid aortic valve from 304 surgical specimens” Sievers, HH., Schmidtke, C. J Thorac Cardiovasc Surg 2007;133:1226-33
3. “Bicuspid Aortic Valve Disease” Siu, SC, Silversides, CK. JACC Vol. 55, No. 25, 2010:2789 – 800
4. “Bicuspid aortic valve aortopathy in adults: Incidence, etiology, and clinical significance” Int J Card 2015:1;400-407
5. ”Sutureless valve in freestyle root: new surgical valve-in-valve therapy” Villa E, Messina A et al. Ann Thorac Surg 2013:96:e155–e157
6.” Sutureless aortic bioprosthesis valve implantation and bicuspid valve anatomy: an unsolved dilemma?” Lona, M, Guichard JB, et al Heart vessels 2016.31:1783-1789
- Details
- Written by: Efrain A. Miranda, Ph.D.
- Hits: 142680
This is the most popular article on this blog by far! Look at the hits counter above...
Let us know other topics that may interest you in our "Contact Us" page.

Click for a larger image
The ligament of Treitz is formed by a fold of peritoneum over the suspensory muscle of the duodenum. This muscle is also known as the "muscle of Treitz" or "musculus suspensorius duodenii". It was first described in 1853 by Dr. Václav Treitz.
The muscle (see the first image) has an unusual structure in that it is formed by a tendon with two muscular ends of dissimilar embryological origin and function. The superior muscular component is skeletal (voluntary) muscle and arises as a slip of muscle (Hilfsmuskel) from the right esophageal crus of the respiratory diaphragm, as well as muscular and ligamentous fibers arising in the region of origin of the celiac trunk and superior mesenteric artery. The inferior portion of the muscle is smooth (involuntary) muscle and has been described as continuous with both the longitudinal and circular muscle layers of the intestine at the duodenojejunal junction.
The ligament of Treitz is an anatomical landmark used by anatomists and surgeons to denote the duodenojejunal junction and the point where the small intestine passes from retroperitoneal duodenum to intraperitoneal jeunum. Surgeons use the ligament of Treitz to measure the jejunum to decide where to perform an anastomosis.

Original image of the "ligament of Treiz"
There is much discussion today on eponyms, that is, associating an individual's name to an anatomical structure or surgical procedure. In spite of the pressure to make eponyms dissapear, the ligament of Treitz is here to stay!
The second image is a copy of the original image published by Dr. Václav Treitz in his 1853 publication "Ueber einen neuen Muskel am Duodenum des Menschens" (On a new muscle in the duodenum of man). The 'muscle of Treitz" is marked by an arrow.
It is important to clarify that the term "ligament" in the abdominopelvic cavity has a different meaning and structure from a skeletal ligament found in a joint. For more information click here. The term "Ligament of Treitz" refers to the fold of peritoneum that attaches to the posterior aspect of the abdominal and lines the "muscle of Treitz".
Clinical anatomy, pathology, and surgery of the gastrointestinal tract are some of the many lecture topics developed and delivered to the medical devices industry by Clinical Anatomy Associates, Inc.
Sources:
1. "Clinically Oriented Anatomy" Moore, KL. 3r Ed. Williams & Wilkins 1992
2. "The origin of Medical Terms" Skinner, AH, 1970
3. "The suspensory muscle of the duodenum and its nerve supply" Jit, I.; Singh, S. J. Anat. (1977), 123, 2, pp. 397-405
4. "Anatomical and functional aspects of the human suspensory muscle of the duodenum." Costacurta, L. Acta Anat (Basel). 1972;82(1):34-46
Image property of: CAA.Inc. Artists: Dr. E. Miranda and D.M. Klein
- Details
- Written by: Efrain A. Miranda, Ph.D.
Interleaflet triangles of the aortic valve by MTD.
Click for a larger image.
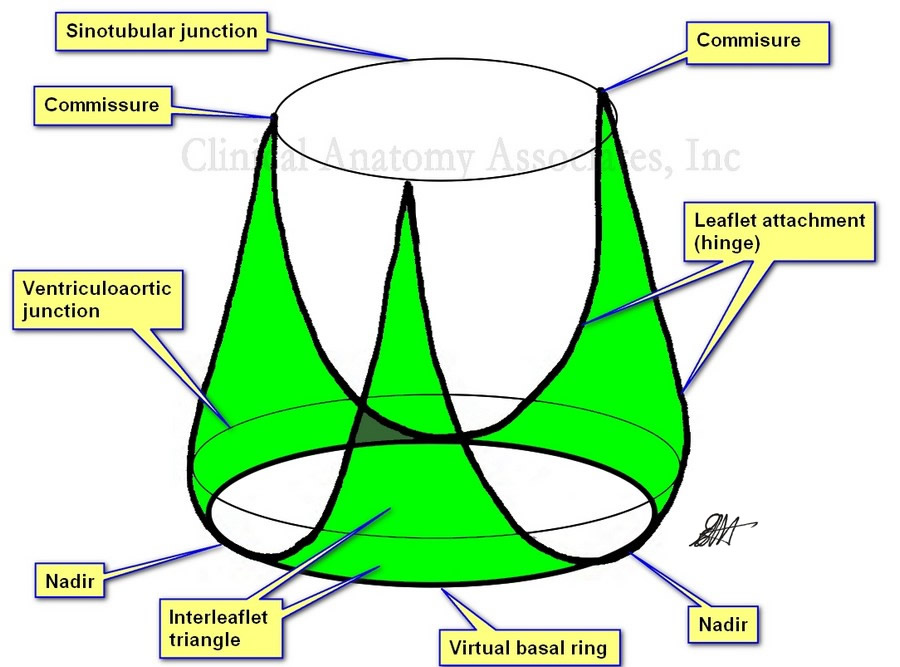
The interleaflet triangles (ILTs) are three triangular regions found in the ventricular aspect of the aortic root. They are bound inferiorly by the virtual basal ring (VBR), laterally by the attachment of the leaflets (the hinge) to the aorta and left ventricular wall (muscular and fibrous), and superiorly by the commissures (site of attachment and meeting of adjacent leaflets) which are usually located at the sinotubular junction, also known as the sinotubular ridge.
A review of the literature on the topic shows that although many speak of these ILTs, not many authors have clearly defined their boundaries. In fact, some only reserve the term ILT to the triangular region distal to the ventriculoaortic boundary. The description used in this article includes the ventricular wall found between the VBR and the ventriculoaortic junction as well as fibrous components found between these two boundaries. Based on this description, we have developed an image of the ILTs that, to our knowledge is not found in literature. (see accompanying images).
The virtual basal ring is a circular virtual line formed by the nadirs of the three aortic leaflets (cusps). The attachment of the three leaflets create a three-pronged coronet that is useful in defining the interleaflet triangles (see image)
The superior boundary of the ILTs is formed by three commissures, the points where the leaflets meet each other at the sinotubular junction. There are two posterior commissures, right and left. The right-posterior commissure is found between the noncoronary and the left coronary sinuses (of Valsalva). An important point about this commissure is that it is situated above the midpoint of the septal (anterior) leaflet of the mitral valve. The left-posterior commissure is found between the left and the right coronary sinuses. The anterior commissure is located between the right and the noncoronary sinus close to the membranous interventricular septum.
Based on the above description, there are three interleaflet triangles:
a. Right (posterior), left (posterior), and anterior. The right posterior ILT is located between the noncoronary and the left coronary sinuses, and just as the commissure at its apex, is located at the midpoint of the septal (anterior) leaflet of the mitral valve. Also, the superior aspect of this ILT is related to the transverse pericardial sinus.
b. The left posterior ILT is located between the right and the left coronary sinuses, and is lies immediately behind the right ventricular outlet.
c. The anterior ILT is found between the right and the noncoronary sinuses. It is related to the membranous septum and the right fibrous trigone, forming part of the central fibrous body (skeleton) of the heart. This ILT is a good anatomical landmark to the location of the bundle of His and the left bundle branch, both components of the conduction system of the heart. These structures can be compressed during the implantation of an aortic or mitral valve, causing transitory or permanent cardiac conduction problems.
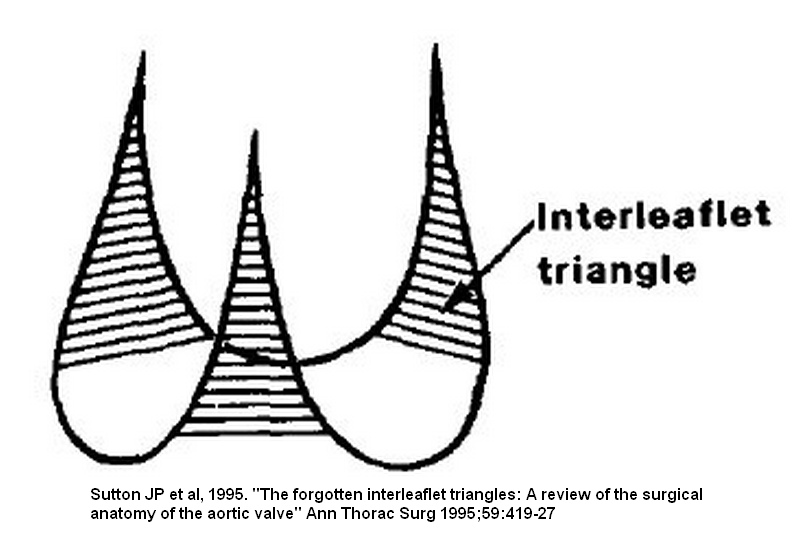
Interleaflet triangles of the aortic valve by Sutton.
Click for a larger image.
The ILTs are important in the normal physiology and hemodynamics of the aortic valve. A small ILT will affect the diameter of the valve and the movement of the leaflets, causing stenosis. This is the case in bicuspid aortic valves where the fusion of two of the leaflets leads to the reduction in size of the ILT normally found between these two fused leaflets.
Since they are located within the functional portion of the left ventricle, the ILTs are subject to the pressures of the ventricle and can be areas that develop aneurysms.
Because of their importance in the hemodynamics of the aortic valve, new procedures and medical devices that reshape the ILTs are being developed. This is specially important in the case of a bicuspid aortic valve, where the interleaflet triangles may be abnormal.
Further to the images that are depicted in this article, the lower image is the classic image of the interleaflet triangles by Sutton (1995). As you can see, the base of the triangles is shown straight with no clear boundary, and it seems as though they are related to the ventriculoaortic junction. The nadirs are not used as a point of reference. The upper image (developed by us and based on Sutton's original sketch) clearly shows the extent of the ILTs as well as their relation to the three landmarks that define the aortic root: The virtual basal ring, the ventriculoaortic junction, and the sinotubular junction.
NOTE: The pulmonary valve also has interleaflet triangles, with a somewhat similar description, but since they are under low pressure they do not develop or are cause of pathology as the ILTs of the aortic valve.
Sources:
1. The Anatomy of the Aortic Root: Loukas, M et al. Clinical Anatomy 27:748–756 (2014)
2. “Extracardiac aneurysm of the interleaflet triangle above the aortic-mitral curtain due to infective endocarditis of the bicuspid aortic valve.” Hori D, et al. Gen Thorac Cardiovasc Surg. 2008 Aug;56(8):424-6
3. “Anatomy of the aortic root: implications for valve-sparing surgery” Efstratios I. Charitos, HS. Ann Cardiothorac Surg 2013;2(1):53-56
4. “The Forgotten Interleaflet Triangles: A Review of the Surgical Anatomy of the Aortic Valve” Sutton JP, et al Ann Thorac Surg 1995;59:419-27
5.” The aortic interleaflet triangles annuloplasty: a multidisciplinary appraisal” Mangini, A., et al. European Journal of Cardio-Thoracic Surgery, Vol. 40:4, 2011, 851-857
6. “Structure and Anatomy of the Aortic Root” Ho, SH., Eur J Electrocar 2009 10; i3-i10
7. “In vitro study of the aortic interleaflet triangle reshaping” Vismara, R Journal of Biomechanics; 47:2; 2014. 329-33
- Details
- Written by: Efrain A. Miranda, Ph.D.

Aortic root and aortic valve.
Click for a larger image.
This article is a continuation of: The aortic root and the aortic valve (1)
The aortic valve is formed by three semilunar leaflets which are very thin as to be almost transparent. The attachment of the leaflets is complex, as part of them attaches to ventricular wall, part attaches to the sinusal arterial wall, and even part of them attaches to the membranous interventricular septum and other fibrous structures. Loukas et al state that at “least one third of the circumference of the aortic root is supported by fibrous tissue rather than ventricular musculature”
Each of the three aortic leaflets has a semilunar attachment and shape (hence the term “semilunar valve” used for both the aortic and pulmonary valve, as they have similar shape). The attachment of these three leaflets create a continuous line where the highest points are the three locations where the leaflets attach at the STJ, and the three lower points or “nadirs” form an edge shaped like a three-pronged “coronet”. This coronet is called by many the “anatomical anulus” of the aortic valve, as this is where the fibrous skeleton of the heart forms the “hinges” of the aortic valve.
The leaflets of the aortic valve (as well as those in the pulmonary valve) have a tissue excrescence that can become quite hard at the point where the three leaflets touch on each heartbeat. These are the nodules of Arantius, named after Giulio Cesare Aranzio (1530 – 1589). As a side note, the nodules of the pulmonary valve have a different name. Distally, the aortic leaflets may present a very thin extension that may be cribriform (not shown in the sketch). These are called the lunulae (singular: lunula) as they look like a sliver of moon.
The second component of the base of the aortic root is a ring defined by the lowest portion of each leaflet, the nadir. This ring is called the “virtual basal ring”, is found within the left ventricle and is used as a surgical reference for aortic valve replacement implants.
The three leaflets are found within three dilations of the aortic root, each one called a “sinus of Valsalva”, which extend between the virtual basal ring inferiorly and the STJ superiorly. The presence of the sinuses of Valsalva permits “fluttering” of the open aortic leaflets in ventricular systole. This fluttering of the leaflets allows blood to flow into the sinuses and into the coronary arteries during ventricular systole.
Aortic valve may present with different number of leaflets, as in the case of a bicuspid aortic valve.
The shape of the attachment of the leaflets create two distinct situations:
First, there is a portion of the ventricle related to the leaflets where the ventricle acts as an artery, the aorta. These areas are found inside the sinuses of Valsalva.
Second, there are triangular areas of the aortic root (the interleaflet triangles) where the aortic wall is within the left ventricle and submitted to the pressures and hemodynamics of the left ventricle. These interleaflet triangles have been involved in aneurysms. For simplicity, these interleaflet triangles are not shown in the sketch and are the subject of a separate article in this website.
Note: The image depicts only one complete aortic leaflet. The other one has been transected to show the sinus of Valsalva and the third has been removed to show the attachment or "hinge" of the leaflet. For an anatomical image of the aortic valve click here.
Sources:
1. The Anatomy of the Aortic Root: Loukas, M et al. Clinical Anatomy 27:748–756 (2014)
2. “Extracardiac aneurysm of the interleaflet triangle above the aortic-mitral curtain due to infective endocarditis of the bicuspid aortic valve.” Hori D, et al. Gen Thorac Cardiovasc Surg. 2008 Aug;56(8):424-6
3. “Anatomy of the aortic root: implications for valve-sparing surgery” Efstratios I. Charitos, HS. Ann Cardiothorac Surg 2013;2(1):53-56
4. “The Forgotten Interleaflet Triangles: A Review of the Surgical Anatomy of the Aortic Valve” Sutton JP, et al Ann Thorac Surg 1995;59:419-27
Image property of: CAA, Inc. Artist: Dr. Miranda
- Details
- Written by: Efrain A. Miranda, Ph.D.
Aortic root and aortic valve.
Click for a larger image.
The term “aortic valve” refers to the three leaflets (or cusps) components that allow passage of blood from the left ventricle to the ascending aorta during ventricular systole, while at the same time preventing regurgitation or reflux of blood back into the ventricle during ventricular diastole. In reality, the “valve” is only a component of a larger structure called the “aortic root”. This article will describe the components of the aortic root and the aortic valve.
The ascending aorta presents with two distinct segments. The proximal segment is a dilated portion called the aortic root. The distal portion is known as the tubular portion of the ascending aorta. The boundary between these two portions is the [sinotubular junction (STJ). Some authors will recognize as the ascending aorta only the tubular portion.
The aortic root is that portion of the ventricular outflow tract and proximal aorta that supports the leaflets of the aortic valve. It is a functioning unit with relations both to the to the aorta and to the left ventricle, and it is here where in most cases we find the ostia of the right and left coronary arteries.
The aortic root is composed of the three dilated sinuses of Valsalva, two of which give origin to the coronary arteries (right and left), three leaflets (or cusps), and the interleaflet triangles. While the distal boundary of the aortic root is clearly defined (the STJ), the proximal boundary is not as clear and is difficult to define. The STJ is defined by the apices of the three aortic leaflets as well as a clear line that appears as the aorta passes from the dilations of the sinuses of Valsalva to the well-defined tubular portion of the ascending aorta.
This proximal boundary is defined clinically by two circular regions: the ventriculoaortic ring distally and the virtual basal ring proximally.
The ventriculoaortic ring is a circular region formed by the left ventriculoaortic junction (the point where the aorta anchors on the left ventricle), and fibrous tissue of both the “cardiac skeleton” and the membranous interventricular septum. It is also called the “surgical anulus”. This is the area where a surgeon will anchor an aortic replacement valve.
Continued here: The Aortic Root and the Aortic Valve (2)
Note: The image depicts only one complete aortic leaflet. The other one has been transected to show the sinus of Valsalva and the third has been removed to show the attachment or "hinge" of the leaflet. For an anatomical image of the aortic valve click here.
Sources:
1. The Anatomy of the Aortic Root: Loukas, M et al. Clinical Anatomy 27:748–756 (2014)
2. “Extracardiac aneurysm of the interleaflet triangle above the aortic-mitral curtain due to infective endocarditis of the bicuspid aortic valve.” Hori D, et al. Gen Thorac Cardiovasc Surg. 2008 Aug;56(8):424-6
3. “Anatomy of the aortic root: implications for valve-sparing surgery” Efstratios I. Charitos, HS. Ann Cardiothorac Surg 2013;2(1):53-56
4. “The Forgotten Interleaflet Triangles: A Review of the Surgical Anatomy of the Aortic Valve” Sutton JP, et al Ann Thorac Surg 1995;59:419-27
Image property of: CAA, Inc. Artist: Dr. Miranda