![]()
Medical Terminology Daily (MTD) is a blog sponsored by Clinical Anatomy Associates, Inc. as a service to the medical community. We post anatomical, medical or surgical terms, their meaning and usage, as well as biographical notes on anatomists, surgeons, and researchers through the ages. Be warned that some of the images used depict human anatomical specimens.
You are welcome to submit questions and suggestions using our "Contact Us" form. The information on this blog follows the terms on our "Privacy and Security Statement" and cannot be construed as medical guidance or instructions for treatment.
We have 821 guests and no members online
")
Marcia Crocker Noyes
(1869 – 1946)
Further to my comment on old books and research that started with an interesting bookplate (Ex-Libris). I continued my research and found that the person in charge of the Osler library bookplate was a fascinating individual that today maybe a ghost in the MedChi library and building in Baltimore... This is certainly an article that can be called "A Moment in History"
Marcia Crocker Noyes was the librarian at The Maryland State Medical Society from 1896 to 1946 and was a founding member of the Medical Library Association.[1][2][3]
Sir William Osler, MD. a famous Johns Hopkins surgeon was a noted bibliophile and had a large personal collection of books on various topics. When he became the President of MedChi in 1896, he was dismayed at the condition of the library and knew that with the right person and some stewardship, it could become a significant collection. Sir William asked his friend, Dr. Bernard Steiner, a physician and President of the Enoch Pratt Free Library in Baltimore for suggestions of a librarian, and Dr. Steiner recommended Marcia Crocker Noyes. A native of New York, and a graduate of Hunter College, Marcia had moved to Baltimore for a lengthy visit with her sister, and took a “temporary” position at the Pratt Library, which turned into three years. Although she had no medical experience or background, she was enthusiastic, and most importantly, she was willing to move into the apartment provided for the librarian, who needed to be available 24 hours a day.
The image in this article is Ms. Noyes on her first year on the job. Marcia developed a book classification system for medical books, based on the Index Medicus, and called it the Classification for Medical Literature. The system uses the alphabet with capital letters for the major divisions of medicine and lower-case ones for the sub-sections. The system was used for many years, but it's now dated and the Faculty's original shelving scheme was never changed. The card catalogs still reflect her classification and many of the cards are written in Marcia's back-slanting handwriting.
Marcia knew enough to ask the Faculty's members about medical questions, terminology and literature. She gradually won over the predominantly male membership and they became her greatest allies; Sir William at the start, and then for nearly 40 years, Dr. John Ruhräh, a wealthy pediatrician with no immediate family of his own. She made a point of attending almost every Faculty function, and in 1904, under guidelines from the American Medical Association, Marcia was made the Faculty Secretary. For much of her first 10 years, she was the Faculty's only full-time employee, only being assisted by Mr. Caution, the Faculty's janitor. Later in life Marcia would say that she hired him because of his name!
Within ten years, the library had outgrown its space, and plans, spearheaded by Marcia and Sir William before his move to Oxford, were made to build a headquarters building, mainly to house the library's growing collection of medical books and journals.
Marcia was instrumental in the design and building of the new headquarters. She travelled to Philadelphia, New York and Boston to look at their medical society buildings, and eventually, the Philadelphia architectural firm, Ellicott & Emmart was selected to design and build the new Faculty building. Every detail of the building held her imprimatur, from the graceful staircase, to the light-filled reading room, and all of the myriad details of the millwork, marble tesserae, and most of all, the four-story cast iron stacks. She was on-site, climbing up unfinished staircases, checking out the progress of the building, which was built in less than one year at a cost of $90,000.
Among the features of the new building was a fourth-floor apartment for her. She referred to it as the "first penthouse in Baltimore" and it had a garden and rooftop terrace. The library collection eventually grew to more than 65,000 volumes from medical and specialty societies around the world. Journals were traded back and forth, and physicians eagerly anticipated the arrival of each new issue. At the same time, Marcia was involved in the Medical Library Association as one of eight founding members. The MLA promotes medical libraries and the exchange of information. One of the earliest mandates of the MLA was the Exchange, a distribution and trade service for those who had duplicates or little-used books in their collections. Initially, the Exchange was run out of the Philadelphia medical society, but in 1900 it was moved to Baltimore and Marcia oversaw it. Several hundred periodicals and journals were received and sent each month, a huge amount of work for a tiny staff. In 1904, the Faculty had run out of room to manage the Exchange, so it was moved to the Medical Society of the Kings County (Brooklyn). But without Marcia's excellent administrative skills, it floundered and in 1908, the MLA asked Marcia to take charge once again.
In 1909, when the new Faculty building opened, there was enough room to run the Exchange and with the help of MLA Treasurer, noted bibliophile and close friend, Dr. John Ruhräh, it once again became successful. Additionally, Marcia and Dr. Ruhräh combined forces to revive the MLA's bulletin, which had all but ceased publication in 1908, taking the Exchange with it. This duo maintained editorial control from 1911 until 1926. In 1934, around the time of Dr. Ruhräh's death, Marcia became the first “unmedicated” professional to head the MLA. During her tenure, the MLA incorporated, the first seal was adopted, and the annual meeting was held in Baltimore. Marcia wanted to write the history of the MLA once she retired from full-time work at the Faculty, but her health was beginning to fail. She had back problems and had suffered a serious burn on her shoulder as a young woman, possibly from her time running a summer camp, Camp Seyon, for young ladies in the Adirondack Mountains. In 1946, a celebration was planned to honor Marcia's 50 years at the Faculty. But she was adamant that the physicians wait until November, the actual date of her 50 years. However, they knew she was gravely ill, and might not make it until then, so a huge party was held in April. More than 250 physicians attended the celebration, but the ones she was closest to in the early years, were long gone. She was presented with a suitcase, a sum of money to use for travelling, and her favorite painting of Dr. John Philip Smith, a founder of the Medical College in Winchester, Virginia. It was painted by Edward Caledon Smith, a Virginia painter who had been a student of the painter Thomas Sully.[4] She adored this painting and vowed, jokingly, to take it with her wherever she went.
The painting was not to stay with her for very long, for she died in November 1946, and left it to the Faculty in her will. Her funeral was held in the Faculty's Osler Hall, named for her dear friend. More than 60 physicians served as her pallbearers, and she was buried at Baltimore's Green Mount Cemetery. In 1948, the MLA decided to establish an award in the name of Marcia Crocker Noyes. It was for outstanding achievement in medical library field and was to be awarded every two years, or when a truly worthy candidate was submitted. In 2014, the Faculty began giving a bouquet of flowers to the winner of the award in Marcia's name, and in honor of her work. Much evidence exists for this tradition, as we know that the physicians, especially Drs. Osler and Ruhräh, frequently gave her bouquets of flowers. Marcia also cultivated flower gardens at the Faculty and decorated the rooms with her work.
Today, the MedChi building is open for tours and if the rumors are to be believed Ms. Marcia Crocker Noyes is still at work in her beloved library as the "resident ghost" [1][5]

NOTE: This article has been modified from the original Wikipedia article on Marcia Crocker Noyes. The article itself is well-written with interesting images of the subject. I would encourage you to visit it. The second insert is from book 00736 in my personal library and shows in pencil, the incredibly small handwriting of Marsha C. Noyes.
Sources:
1. "Marcia, Marcia, Marcia" MedChi Archives blog.
2. "Marcia C. Noyes, Medical Librarian" (PDF). Bulletin of the Medical Library Association. 35 (1): 108–109. 1947. PMC 194645
3. Smith, Bernie Todd (1974). "Marcia Crocker Noyes, Medical Librarian: The Shaping of a Career" (PDF). Bulletin of the Medical Library Association. 62 (3): 314–324. PMC 198800Freely accessible. PMID 4619344.
4. Edward Caledon BRUCE (1825-1901)"
5. Behind the scenes tour MedChiBuilding
"Clinical Anatomy Associates, Inc., and the contributors of "Medical Terminology Daily" wish to thank all individuals who donate their bodies and tissues for the advancement of education and research”.
Click here for more information
- Details
This article is part of the series "A Moment in History" where we honor those who have contributed to the growth of medical knowledge in the areas of anatomy, medicine, surgery, and medical research.
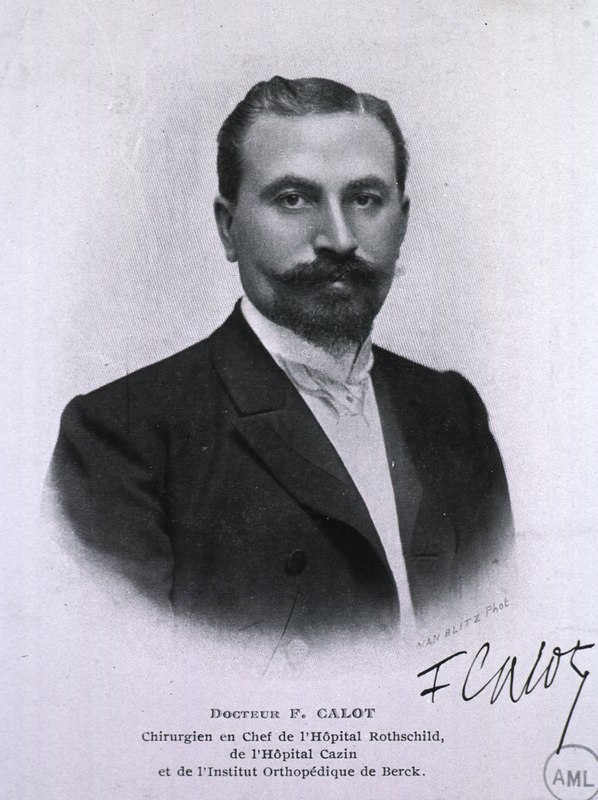
Jean-Francois Calot (1861 – 1944)
Jean-Francois Calot (1861 – 1944). French physician and anatomist, Jean-Francois Calot was born in Arrens-Marsous, a small farming community of the Hautes-Pyrénées. He received his bachelor degree in 1880 at Saint-Pe de Bigorre, and then continued to study Medicine at the University of Paris, where he worked as an anatomy prosector. His doctoral thesis “De La Cholecystectomie” (On Cholecystectomy) was published in 1890 and republished in 1891.
Although his main interest laid in orthopedics and tuberculosis, Calot’s name is eponymically tied to an anatomical landmark described in his thesis, the “Triangle of Calot”, a triangular area that includes the biliary ducts associated with the gallbladder and the vascular supply to the gallbladder. This is an important region because of the high number of anatomical variations found in the area.
There is a discrepancy between the original description of this triangular region by Calot and what is used today. For more information, click on this link to read more on the “Triangle of Calot”, also known as the “cystohepatic triangle”.
During his medical career Calot worked at several French hospitals including the Rothschild hospital where he became Chief of Surgery. He was also the Chief of Surgery for the Cazin-Perrochaud Hospital, and the Orthopedic Institute of Berck-sur-Mer
Dr. Jean-Francois Calot and
the treatment of Pott's disease
During his orthopedic career Calot published many books “Chirurgie et orthopédie de guerre”, “Les maladies qu'on soigne á Berck”, “Berck et ses traitements : les raisons de sa supériorit?”, but his opus magnus is the book “« L'orthopédie indispensable aux praticiens” (Indispensable orthopedics for practitioners).
Calot is also known for his treatment of tuberculotic abscesses, and a conservative approach to musculoskeletal tuberculosis. The surgical approach of the times was to surgically open and clean the tuberculotic bone. Calot is known to have said “Ouvrir la tuberculose, c'est ouvrir la porte d' la mort” (To open the tuberculosis is to open the door to death).
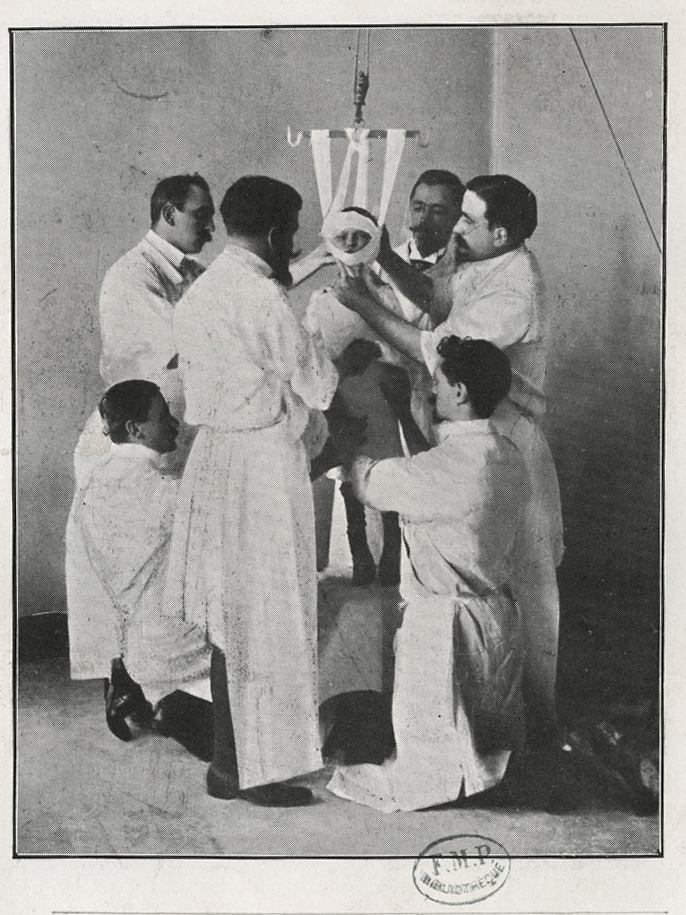
Continuing his studies and treatment of tuberculosis, on December 22nd, 1896 Calot presents the the French Academy of Medicine a study of the treatment of 37 patients with hyperkyphosis due to Pott’s disease, a tuberculotic spinal deformity, named after Sir Percival Pott. This method included traction and a brace. The second image shows this treatment. Dr. Calot is standing at the center, looking at the patient.
In 1900 Calot founded the “Orthopedic Institute of Berck” which today is known as “Calot’s Institute of Berck-sur-Mer”.
Sources:
1. “Calot's triangle” Abdalla S, Pierre S, Ellis H. Clin Anat. 2013 May;26 (4):493-501
2. “La Vie et l'OEuvre de Francois Calot, chirurgien orthopédiste de Berck” Loisel, P. (in French). Report presented at Société Francaise d'Histoire de la Médecine on 18 March 1987
Image 1: Original image courtesy of the National Library of Medicine
Image 2: Original image public domain courtesy of the Universite Paris-Descartes Histoire de la Santé
- Details
UPDATED: This is a word based on the Greek term [νευρών] (nevrón), which was used initially to denote or mean "sinew" or "tendon". The early descriptions of anatomy made no difference between a nerve and a tendon. The meaning of the word [aponeurosis], although not exactly literal, is that of a "flat tendon".
This is important in abdominal wall anatomy and to understand the anatomy of the inguinofemoral region as it relates to hernia. There are three aponeuroses (plural form), the external oblique aponeurosis, the internal oblique aponeurosis, and the transversus abdominis aponeurosis, all contributing to the rectus sheath and the linea alba.
There are other aponeuroses in the human body, such as the fascia lata and the superficial and deep gastrocnemius aponeuroses that end in the calcaneal (Achilles) tendon.
- Details

Click for a larger image
The [common hepatic artery] is one of the three branches that arise from the celiac trunk providing blood supply to the liver, duodenum, and pancreas. The common hepatic artery ends where the gastroduodenal artery arises, and then changes its name to proper hepatic artery
It is a relatively short artery, close to 3 cm. in length, with an average diameter of 7 mm.
It can present with simple to complex anatomical variations. In one of them the common hepatic artery arises from the superior mesenteric artery and not from the celiac trunk. For more information on anatomical variations of the celiac trunk and the common hepatic artery click here.
The image shows an anteroinferior view of the liver and stomach, the duodenum and stomach are reflected anteriorly. CT= Celiac trunk, CHA= Common hepatic artery, PHA= Proper hepatic artery, GDA= Gastroduodenal artery
Sources:
1. "Gray's Anatomy"38th British Ed. Churchill Livingstone 1995
2. "Tratado de Anatomia Humana" Testut et Latarjet 8 Ed. 1931 Salvat Editores, Spain
3. "Variations of hepatic artery: anatomical study on cadavers" Sebben, GA et al Rev. Col. Bras. Cir. 40:3 May/June 2013
Image property of: CAA.Inc.Photographer: David M. Klein
- Details
UPDATED: The root term for this word comes from the Latin [fenestram] meaning "window". [Fenestration] is "the presence or the act of creating a window". As an example, the term is used to describe a small, round opening found in the medial wall of the tympanic cavity (middle ear), the [fenestra cochleae] or [fenestra rotunda] meaning "round window" (see image 1).
") I
I in the cusps of the aortic valve") I
I{kind=link}
Fenestrations can be found as natural occurrences in the body, as a result of an infection or destructive process or pathology, or they can be surgical procedures attempting to create a window, opening, or foramen. The cusps of all the heart valves can present normal fenestrations in the distal aspect of the cusp, beyond the coaptation or closure line. These become abnormal fenestrations when they occur below the coaptation line which may need to be repaired. Image 2 shows normal and abnormal fenestrations in the cusps of an aortic valve. Fenestrations in a valve cusp can be caused by endocarditis, among other causes.
Some surgical fenestrations that can be described are:
1. Fenestration of a tooth, allowing for drainage.
2. Pericardial fenestration, also known as a "pericardial window" to allow for drainage of excessive pericardial fluid (pericardial effusion).
3. Fenestration in a Fontan procedure, where a small opening or "window" is created to relieve excessive pressure in the venous circulation.
Word suggested by: J.Estrada
Original image #1courtesy of bartleby.com. Image#2 property of CAA, Inc.Artist: Dr. Miranda
- Details
This medical term [hypoacusia] is composed of the prefix [ hyp-], a derivate from the Greek [υπό] (ip? which means "under", "deficient" or "below". The root term [-acus-] is also a derivate from the Greek [ακούω] (ako?o?) meaning “listen”, or “hear”. The adjectival suffix [-ia] has a double meaning of “pertaining to” and “condition”. The term hypoacusia means then “a condition of deficient hearing”. It can also be used as [hypoacusis] with the same meaning.
A common mistake is to use this term for total deafness. This is not correct, in [hypoacusia] the patient has varying degrees of hearing loss, but there is some hearing function left.
There are many causes of hypoacusia: genetic, viral, bacterial, traumatic, etc. There are two types of hypoacusia. The first one is transmission hypoacusia, where the mechanical system that transmits vibration from the external ear and tympanic membrane (eardrum) to the inner ear can be damaged. The second type is neurosensory hypoacusia, where the components of the inner ear as well as the nerve structures of the vestibulocochlear nerve (VIII cranial nerve) up to and including brain areas related to the hearing process may be damaged.
Different degrees of hypoacusia have been demonstrated to affect proper communication functions and learning. Lower levels of hypoacusia (less than 25%) can be undiagnosed in small children; in fact, there are several studies that prove that the presence of low level hypoacusia in small children is a good predictor of language alteration and learning problems if not diagnosed properly and timely.
My personal thanks to Maria E. Gallegos, Chair of the Speech Pathology School, Iberoamerican University, Santiago Chile, for her help in this article. Dr. Miranda